

Increasing time to operation is associated with decreased survival in patients with a positive FAST examination requiring emergent laparotomy
- PMID: 23778511
- PMCID: PMC3744056
- DOI: 10.1097/TA.0b013e31828fa54e
Increasing time to operation is associated with decreased survival in patients with a positive FAST examination requiring emergent laparotomy
Abstract
Introduction: Focused assessment with sonography for trauma (FAST) is commonly used to facilitate the timely diagnosis of life-threatening hemorrhage in injured patients. Most patients with positive findings on FAST require laparotomy. Although it is assumed that an increasing time to operation (T-OR) leads to higher mortality, this relationship has not been quantified. This study sought to determine the impact of T-OR on survival in patients with a positive FAST who required emergent laparotomy.
Methods: We retrospectively analyzed patients from the PRospective Observational Multicenter Major Trauma Transfusion (PROMMTT) study who underwent laparotomy within 90 minutes of presentation and had a FAST performed. Cox proportional hazards models including Injury Severity Score (ISS), age, base deficit, and hospital site were created to examine the impact of increasing T-OR on in-hospital survival at 24 hours and 30 days. The impact of time from the performance of the FAST examination to operation (TFAST-OR) on in-hospital mortality was also examined using the same model.
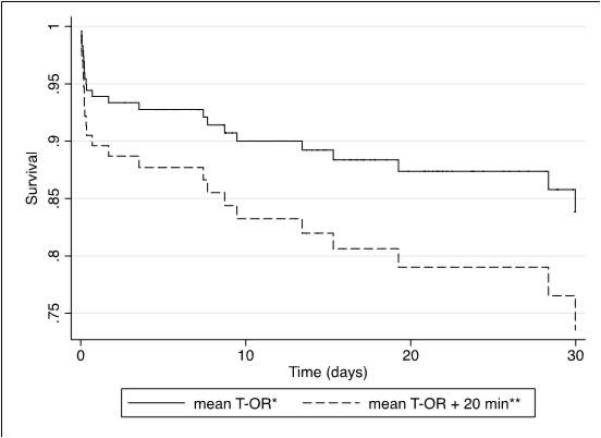
Results: One hundred fifteen patients met study criteria and had complete data. Increasing T-OR was associated with increased in-hospital mortality at 24 hours (hazard ratio [HR], 1.50 for each 10-minute increase in T-OR; confidence interval [CI], 1.14-1.97; p = 0.003) and 30 days (HR, 1.41; CI, 1.18-2.10; p = 0.002). Increasing TFAST-OR was also associated with higher in-hospital mortality at 24 hours (HR, 1.34; CI, 1.03-1.72; p = 0.03) and 30 days (HR, 1.40; CI, 1.06-1.84; p = 0.02).
Conclusion: In patients with a positive FAST who required emergent laparotomy, delay in operation was associated with increased early and late in-hospital mortality. Delays in T-OR in trauma patients with a positive FAST should be minimized.
Figures
References
-
- Committee on Injury Prevention and Control; Institute of MedicineBonne RJ, Fulco CE, Liverman CT, editors. Reducing the Burden of Injury: Advancing Prevention and Treatment. National Academy Press; Washington, DC: 1999. pp. 42–43. - PubMed
-
- American College of Surgeons Committee on Trauma . Resources for Optimal Care of the Injured Patient. American College of Surgeons; Chicago: 2006.
-
- Hemmila MR, Nathens AB, Shafi S, et al. The Trauma Quality Improvement Program: pilot study and initial demonstration of feasibility. J Trauma. 2010;68(2):253–262. - PubMed
-
- Stelfox HT, Bobranska-Artiuch B, Nathens A, et al. Quality indicators for evaluating trauma care. A scoping review. Arch Surg. 2010;145:286–295. - PubMed
-
- Wright KD, Knowles CGH, Coats TJ, et al. Efficient timely evacuation of intracranial haematoma – the effect of transport direct to a specialist centre. Injury. 1996;27:719–721. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
