

A latent class model for defining severe hemorrhage: experience from the PROMMTT study
- PMID: 23778516
- PMCID: PMC3744183
- DOI: 10.1097/TA.0b013e31828fa3d3
A latent class model for defining severe hemorrhage: experience from the PROMMTT study
Abstract
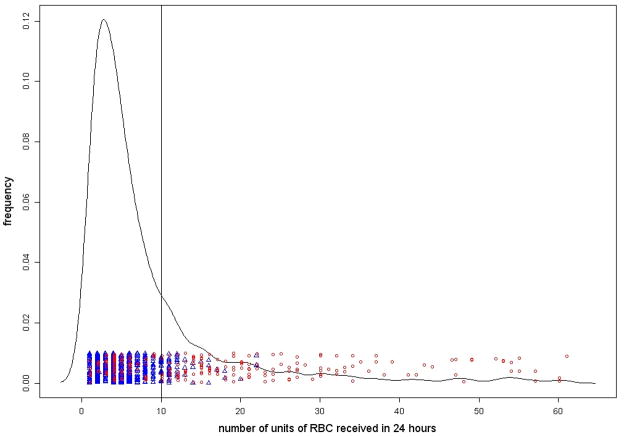
Background: Several predictive models have been developed to identify trauma patients who have had severe hemorrhage (SH) and may need a massive transfusion (MT) protocol. However, almost all these models define SH as the transfusion of 10 or more units of red blood cells (RBCs) within 24 hours of emergency department admission (also known as MT). This definition excludes some patients with SH, especially those who die before a 10th unit of RBCs could be transfused, which calls the validity of these prediction models into question. We show how a latent class model could improve the accuracy of identifying the SH patients.
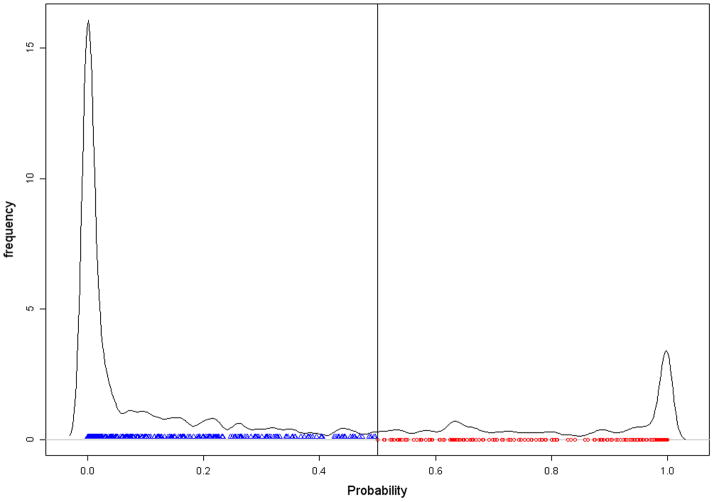
Methods: Modeling SH classification as a latent variable, we estimate the posterior probability of a patient in SH based on emergency department admission variables (systolic blood pressure, heart rate, pH, hemoglobin), the 24-hour blood product use (plasma/RBC and platelet/RBC ratios), and 24-hour survival status. We define the SH subgroup as those having a posterior probability of 0.5 or greater. We compare our new classification of SH with that of the traditional MT using data from PROMMTT study.
Results: Of the 1,245 patients, 913 had complete data, which were used in the latent class model. About 25.3% of patients were classified as SH. The overall agreement between the MT and SH classifications was 83.8%. However, among 49 patients who died before receiving the 10th unit of RBCs, 41 (84%) were classified as SH. Seven (87.5%) of the remaining eight patients who were not classified as SH had head injury.
Conclusion: Our definition of SH based on the aforementioned latent class model has an advantage of improving on the traditional MT definition by identifying SH patients who die before receiving the 10th unit of RBCs. We recommend further improvements to more accurately classify SH patients, which could replace the traditional definition of MT for use in developing prediction algorithms.
Conflict of interest statement
Figures
References
-
- McLaughlin DF, Niles SE, Salinas J, et al. A predictive model for massive transfusion in combat casualty patients. J Trauma. 2008;64:S57–S63. - PubMed
-
- Yucel N, Lefering R, Maegele M, et al. Trauma Associated Severe Hemorrhage (TASH)-Score: probability of mass transfusion as surrogate for life threatening hemorrhage after multiple trauma. J Trauma. 2006;60:1228–1236. - PubMed
-
- Nunez TC, Voskresensky IV, Dossett LA, Shinall R, Dutton WD, Cotton BA. Early prediction of massive transfusion in trauma: simple as ABC (assessment of blood consumption)? J Trauma. 2009;66:346–352. - PubMed
-
- Cotton BA, Dossett LA, Au BK, Nunez TC, Robertson AM, Young PP. Room for (performance) improvement: provider-related factors associated with poor outcomes in massive transfusion. J Trauma. 2009;67:1004–1012. - PubMed
-
- Riskin DJ, Tsai TC, Riskin L, et al. Massive transfusion protocols: the role of aggressive resuscitation versus product ratio in mortality reduction. J Am Coll Surg. 2009;209:198–205. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
