

Hospital outbreak of Middle East respiratory syndrome coronavirus
- PMID: 23782161
- PMCID: PMC4029105
- DOI: 10.1056/NEJMoa1306742
Hospital outbreak of Middle East respiratory syndrome coronavirus
Erratum in
- N Engl J Med. 2013 Aug 29;369(9):886
Abstract
Background: In September 2012, the World Health Organization reported the first cases of pneumonia caused by the novel Middle East respiratory syndrome coronavirus (MERS-CoV). We describe a cluster of health care-acquired MERS-CoV infections.
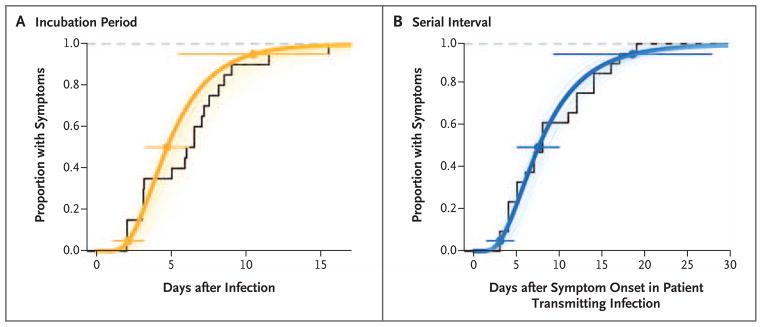
Methods: Medical records were reviewed for clinical and demographic information and determination of potential contacts and exposures. Case patients and contacts were interviewed. The incubation period and serial interval (the time between the successive onset of symptoms in a chain of transmission) were estimated. Viral RNA was sequenced.
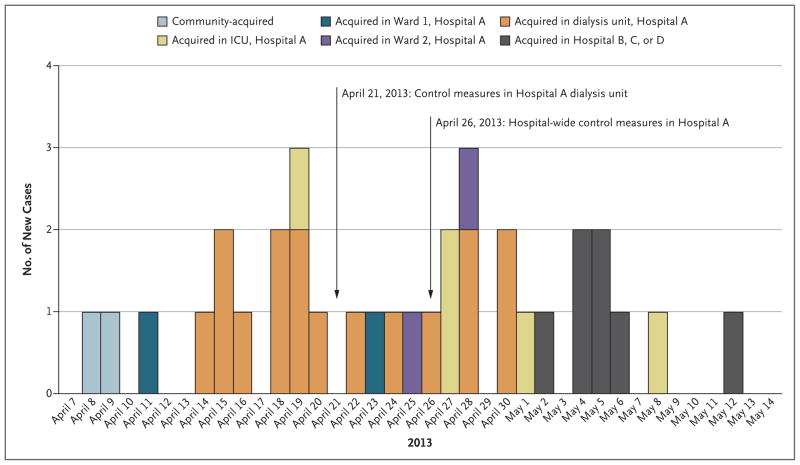
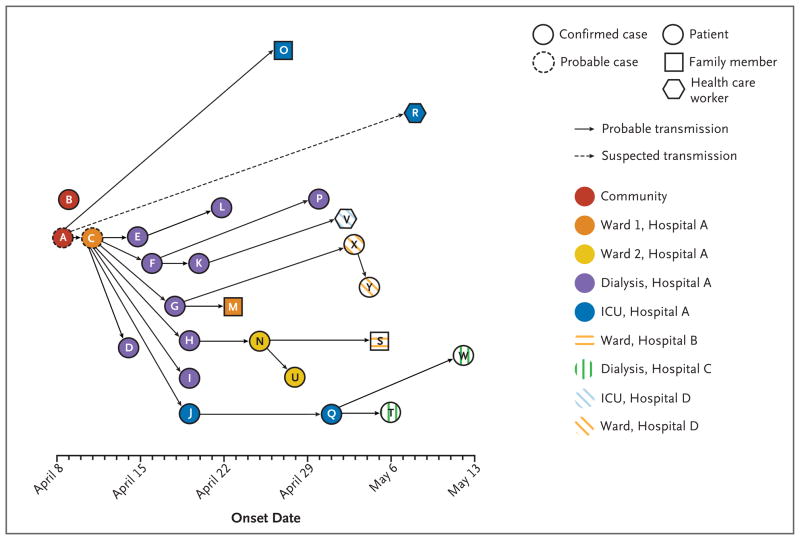
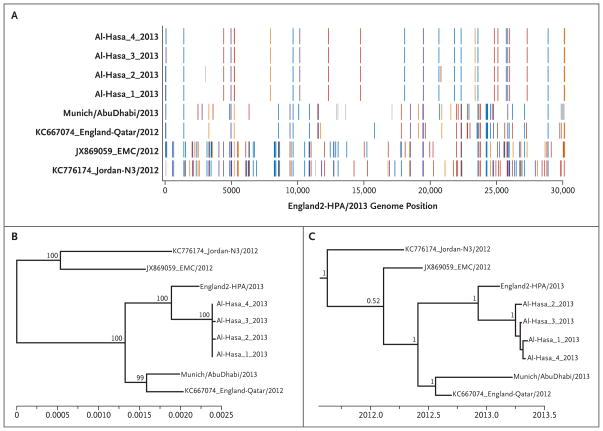
Results: Between April 1 and May 23, 2013, a total of 23 cases of MERS-CoV infection were reported in the eastern province of Saudi Arabia. Symptoms included fever in 20 patients (87%), cough in 20 (87%), shortness of breath in 11 (48%), and gastrointestinal symptoms in 8 (35%); 20 patients (87%) presented with abnormal chest radiographs. As of June 12, a total of 15 patients (65%) had died, 6 (26%) had recovered, and 2 (9%) remained hospitalized. The median incubation period was 5.2 days (95% confidence interval [CI], 1.9 to 14.7), and the serial interval was 7.6 days (95% CI, 2.5 to 23.1). A total of 21 of the 23 cases were acquired by person-to-person transmission in hemodialysis units, intensive care units, or in-patient units in three different health care facilities. Sequencing data from four isolates revealed a single monophyletic clade. Among 217 household contacts and more than 200 health care worker contacts whom we identified, MERS-CoV infection developed in 5 family members (3 with laboratory-confirmed cases) and in 2 health care workers (both with laboratory-confirmed cases).
Conclusions: Person-to-person transmission of MERS-CoV can occur in health care settings and may be associated with considerable morbidity. Surveillance and infection-control measures are critical to a global public health response.
Figures
Comment in
-
Person-to-person spread of the MERS coronavirus--an evolving picture.N Engl J Med. 2013 Aug 1;369(5):466-7. doi: 10.1056/NEJMe1308724. N Engl J Med. 2013. PMID: 23902487 No abstract available.
-
Hospital-associated Middle East respiratory syndrome coronavirus infections.N Engl J Med. 2013 Oct 31;369(18):1761-2. doi: 10.1056/NEJMc1311004. N Engl J Med. 2013. PMID: 24171524 No abstract available.
-
Hospital-associated Middle East respiratory syndrome coronavirus infections.N Engl J Med. 2013 Oct 31;369(18):1761. doi: 10.1056/NEJMc1311004. N Engl J Med. 2013. PMID: 24171525 No abstract available.
References
-
- Peiris JS, Yuen KY, Osterhaus ADME, Stöhr K. The severe acute respiratory syndrome. N Engl J Med. 2003;349:2431–41. - PubMed
-
- Rota PA, Oberste MS, Monroe SS, et al. Characterization of a novel coronavirus associated with severe acute respiratory syndrome. Science. 2003;300:1394–9. - PubMed
-
- Drosten C, Günther S, Preiser W, et al. Identification of a novel coronavirus in patients with severe acute respiratory syndrome. N Engl J Med. 2003;348:1967–76. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous