

Retinopathy of prematurity
- PMID: 23782686
- PMCID: PMC4389630
- DOI: 10.1016/S0140-6736(13)60178-6
Retinopathy of prematurity
Abstract
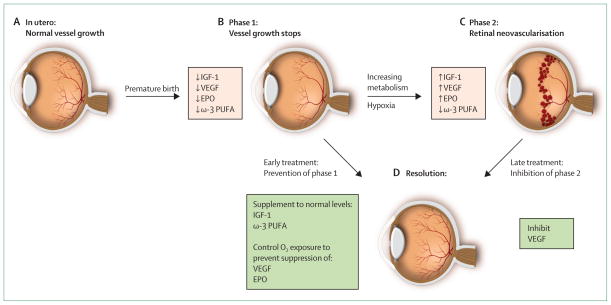
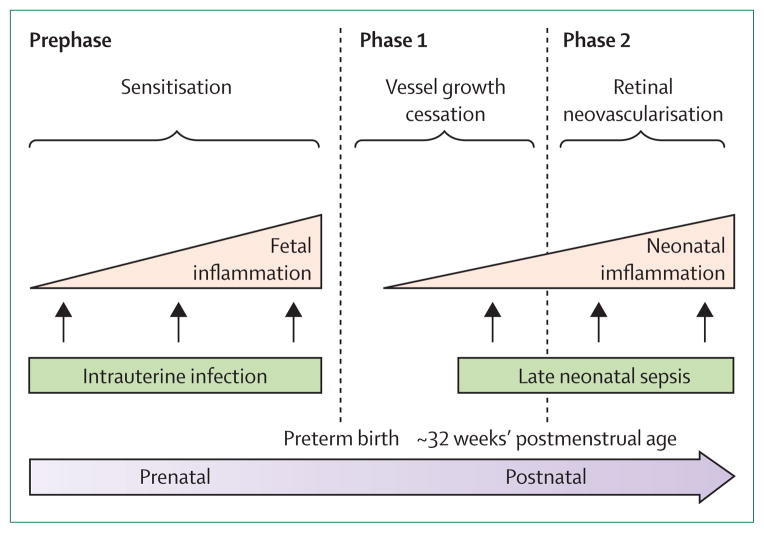
The immature retinas of preterm neonates are susceptible to insults that disrupt neurovascular growth, leading to retinopathy of prematurity. Suppression of growth factors due to hyperoxia and loss of the maternal-fetal interaction result in an arrest of retinal vascularisation (phase 1). Subsequently, the increasingly metabolically active, yet poorly vascularised, retina becomes hypoxic, stimulating growth factor-induced vasoproliferation (phase 2), which can cause retinal detachment. In very premature infants, controlled oxygen administration reduces but does not eliminate retinopathy of prematurity. Identification and control of factors that contribute to development of retinopathy of prematurity is essential to prevent progression to severe sight-threatening disease and to limit comorbidities with which the disease shares modifiable risk factors. Strategies to prevent retinopathy of prematurity will depend on optimisation of oxygen saturation, nutrition, and normalisation of concentrations of essential factors such as insulin-like growth factor 1 and ω-3 polyunsaturated fatty acids, as well as curbing of the effects of infection and inflammation to promote normal growth and limit suppression of neurovascular development.
Copyright © 2013 Elsevier Ltd. All rights reserved.
Conflict of interest statement
AH previously owned shares in PremaCure Holding, which controlled PremaCure (Uppsala, Sweden), a company that had rights to the WINROP system and held patents and patent applications that covered prevention of retinopathy of prematurity with insulin-like growth factor 1. LEHS and OD declare that they have no conflicts of interest.
Figures
References
-
- Silverman WA. Retrolental fibroplasia: a modern parable. New York: Grune & Stratton; 1980.
-
- Campbell K. Intensive oxygen therapy as a possible cause of retrolental fibroplasias: a clinical approach. Med J Aust. 1951;2:48–50. - PubMed
-
- Stenson B, Brocklehurst P, Tarnow-Mordi W. Increased 36-week survival with high oxygen saturation target in extremely preterm infants. N Engl J Med. 2011;364:1680–82. - PubMed
-
- Chen J, Smith LE. Retinopathy of prematurity. Angiogenesis. 2007;10:133–40. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
