

Continuous renal replacement therapy outcomes in acute kidney injury and end-stage renal disease: a cohort study
- PMID: 23782899
- PMCID: PMC4057378
- DOI: 10.1186/cc12780
Continuous renal replacement therapy outcomes in acute kidney injury and end-stage renal disease: a cohort study
Abstract
Introduction: Continuous renal replacement therapy (CRRT) is a widely used but resource-intensive treatment. Despite its broad adoption in intensive care units (ICUs), it remains challenging to identify patients who would be most likely to achieve positive outcomes with this therapy and to provide realistic prognostic information to patients and families.
Methods: We analyzed a prospective cohort of all 863 ICU patients initiated on CRRT at an academic medical center from 2008 to 2011 with either new-onset acute kidney injury (AKI) or pre-admission end-stage renal disease (ESRD). We examined in-hospital and post-discharge mortality (for all patients), as well as renal recovery (for AKI patients). We identified prognostic factors for both in-hospital and post-discharge mortality separately in patients with AKI or ESRD.
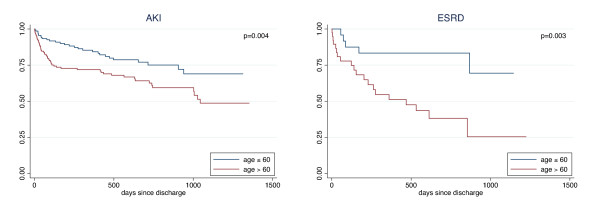
Results: In-hospital mortality was 61% for AKI and 54% for ESRD. In patients with AKI (n=725), independent risk factors for mortality included age over 60 (OR 1.9, 95% CI 1.3, 2.7), serum lactate over 4 mmol/L (OR 2.2, 95% CI 1.5, 3.1), serum creatinine over 3 mg/dL at time of CRRT initiation (OR 0.63, 95% CI 0.43, 0.92) and comorbid liver disease (OR 1.75, 95% CI 1.1, 2.9). Among patients with ESRD (n=138), liver disease was associated with increased mortality (OR 3.4, 95% CI 1.1, 11.1) as was admission to a medical (vs surgical) ICU (OR 2.2, 95% CI 1.1, 4.7). Following discharge, advanced age became a predictor of mortality in both groups (AKI: HR 1.9, 95% CI 1.2, 3.0; ESRD: HR 4.1, 95% CI 1.5, 10.9). At the end of the study period, only 25% (n=183) of patients with AKI achieved dialysis-free survival.
Conclusions: Among patients initiating CRRT, risk factors for mortality differ between patients with underlying ESRD or newly acquired AKI. Long-term dialysis-free survival in AKI is low. Providers should consider these factors when assessing prognosis or appropriateness of CRRT.
Figures
References
-
- Srisawat N, Lawsin L, Uchino S, Bellomo R, Kellum JA. BEST Kidney Investigators. Cost of acute renal replacement therapy in the intensive care unit: results from The Beginning and Ending Supportive Therapy for the Kidney (BEST Kidney) study. Crit Care. 2010;17:R46. doi: 10.1186/cc8933. - DOI - PMC - PubMed
-
- Tumlin JA, Chawla L, Tolwani AJ, Mehta R, Dillon J, Finkel KW, Dasilva JR, Astor BC, Yevzlin AS, Humes HD. The effect of the selective cytopheretic device on acute kidney injury outcomes in the intensive care unit: a multicenter pilot study. Semin Dial. 2012. doi: 10.1111/sdi.12032. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
