

A new risk scheme to predict ischemic stroke and other thromboembolism in atrial fibrillation: the ATRIA study stroke risk score
- PMID: 23782923
- PMCID: PMC3698792
- DOI: 10.1161/JAHA.113.000250
A new risk scheme to predict ischemic stroke and other thromboembolism in atrial fibrillation: the ATRIA study stroke risk score
Abstract
Background: More accurate and reliable stroke risk prediction tools are needed to optimize anticoagulation decision making in patients with atrial fibrillation (AF). We developed a new AF stroke prediction model using the original Anticoagulation and Risk Factors in Atrial Fibrillation (ATRIA) AF cohort and externally validated the score in a separate, contemporary, community-based inception AF cohort, ATRIA-Cardiovascular Research Network (CVRN) cohort.
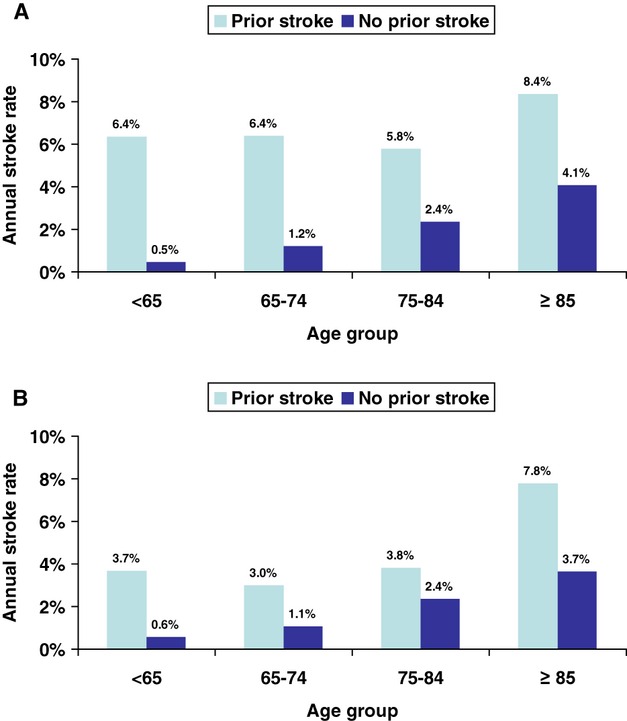
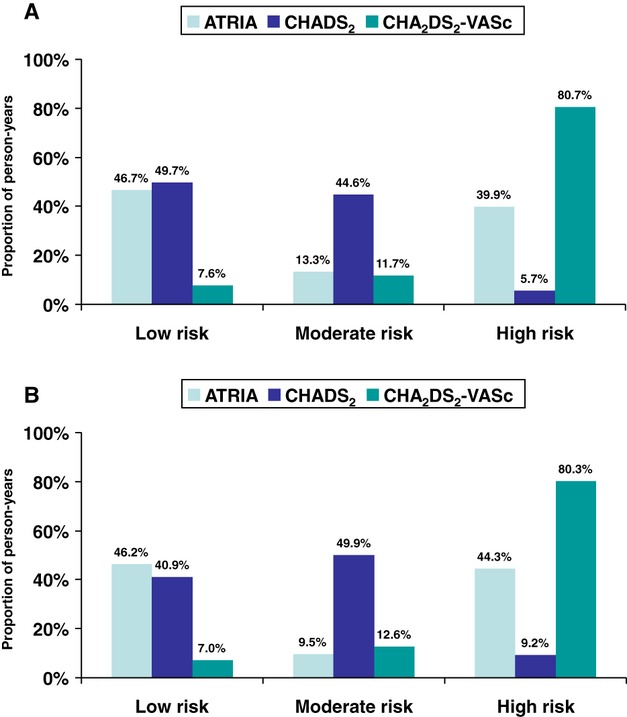
Methods and results: The derivation ATRIA cohort consisted of 10 927 patients with nonvalvular AF contributing 32 609 person-years off warfarin and 685 thromboembolic events (TEs). The external validation ATRIA-CVRN cohort included 25 306 AF patients contributing 26 263 person-years off warfarin and 496 TEs. Cox models identified 8 variables, age, prior stroke, female sex, diabetes mellitus, heart failure, hypertension, proteinuria, and eGFR<45 mL/min per 1.73 m(2) or end-stage renal disease, plus an age×prior stroke interaction term for the final model. Point scores were assigned proportional to model coefficients. The c-index in the ATRIA cohort was 0.73 (95% CI, 0.71 to 0.75), increasing to 0.76 (95% CI, 0.74 to 0.79) when only severe events were considered. In the ATRIA-CVRN, c-indexes were 0.70 (95% CI, 0.67 to 0.72) and 0.75 (95% CI, 0.72 to 0.78) for all events and severe events, respectively. The C-index was greater and net reclassification improvement positive comparing the ATRIA score with the CHADS2 or CHA2DS2-VASc scores.
Conclusions: The ATRIA stroke risk score performed better than existing risk scores, was validated successfully, and showed improvement in predicting severe events, which is of greatest concern. The ATRIA score should improve the antithrombotic decision for patients with AF and should provide a secure foundation for the addition of biomarkers in future prognostic models.
Keywords: anticoagulants; atrial fibrillation; risk score; stroke.
Figures
References
-
- Wolf PA, Abbott RD, Kannel WB. Atrial fibrillation as an independent risk factor for stroke: the Framingham study. Stroke. 1991; 22:983-988 - PubMed
-
- Hart RG, Benavente O, McBride R, Pearce LA. Antithrombotic therapy to prevent stroke in patients with atrial fibrillation: a meta‐analysis. Ann Intern Med. 1999; 131:492-501 - PubMed
-
- Risk factors for stroke and efficacy of antithrombotic therapy in atrial fibrillation. Analysis of pooled data from five randomized controlled trials. Arch Intern Med. 1994; 154:1449-1457 - PubMed
-
- Fuster V, Ryden LE, Cannom DS, Crijns HJ, Curtis AB, Ellenbogen KA, Halperin JL, Le Heuzey JY, Kay GN, Lowe JE, Olsson SB, Prystowsky EN, Tamargo JL, Wann S, Smith SC, Jr, Jacobs AK, Adams CD, Anderson JL, Antman EM, Halperin JL, Hunt SA, Nishimura R, Ornato JP, Page RL, Riegel B, Priori SG, Blanc JJ, Budaj A, Camm AJ, Dean V, Deckers JW, Despres C, Dickstein K, Lekakis J, McGregor K, Metra M, Morais J, Osterspey A, Tamargo JL, Zamorano JL. ACC/AHA/ESC 2006 guidelines for the management of patients with atrial fibrillation: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the European Society of Cardiology Committee for Practice Guidelines (writing committee to revise the 2001 guidelines for the management of patients with atrial fibrillation): developed in collaboration with the European Heart Rhythm Association and the Heart Rhythm Society. Circulation. 2006; 114:e257-e354 - PubMed
-
- Wann LS, Curtis AB, January CT, Ellenbogen KA, Lowe JE, Estes NA, III, Page RL, Ezekowitz MD, Slotwiner DJ, Jackman WM, Stevenson WG, Tracy CM, Fuster V, Ryden LE, Cannom DS, Le Heuzey JY, Crijns HJ, Lowe JE, Curtis AB, Olsson SB, Ellenbogen KA, Prystowsky EN, Halperin JL, Tamargo JL, Kay GN, Wann LS, Jacobs AK, Anderson JL, Albert N, Hochman JS, Buller CE, Kushner FG, Creager MA, Ohman EM, Ettinger SM, Stevenson WG, Guyton RA, Tarkington LG, Halperin JL, Yancy CWACCF/AHA/HRS 2011 ACCF/AHA/HRS focused update on the management of patients with atrial fibrillation (updating the 2006 guideline): a report of the American College of Cardiology Foundation/American Heart Association task force on practice guidelines. J Am Coll Cardiol. 2011; 57:223-242 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
