

Impact of definitions of loss to follow-up on estimates of retention, disease progression, and mortality: application to an HIV program in Mozambique
- PMID: 23785113
- PMCID: PMC3755641
- DOI: 10.1093/aje/kwt030
Impact of definitions of loss to follow-up on estimates of retention, disease progression, and mortality: application to an HIV program in Mozambique
Abstract
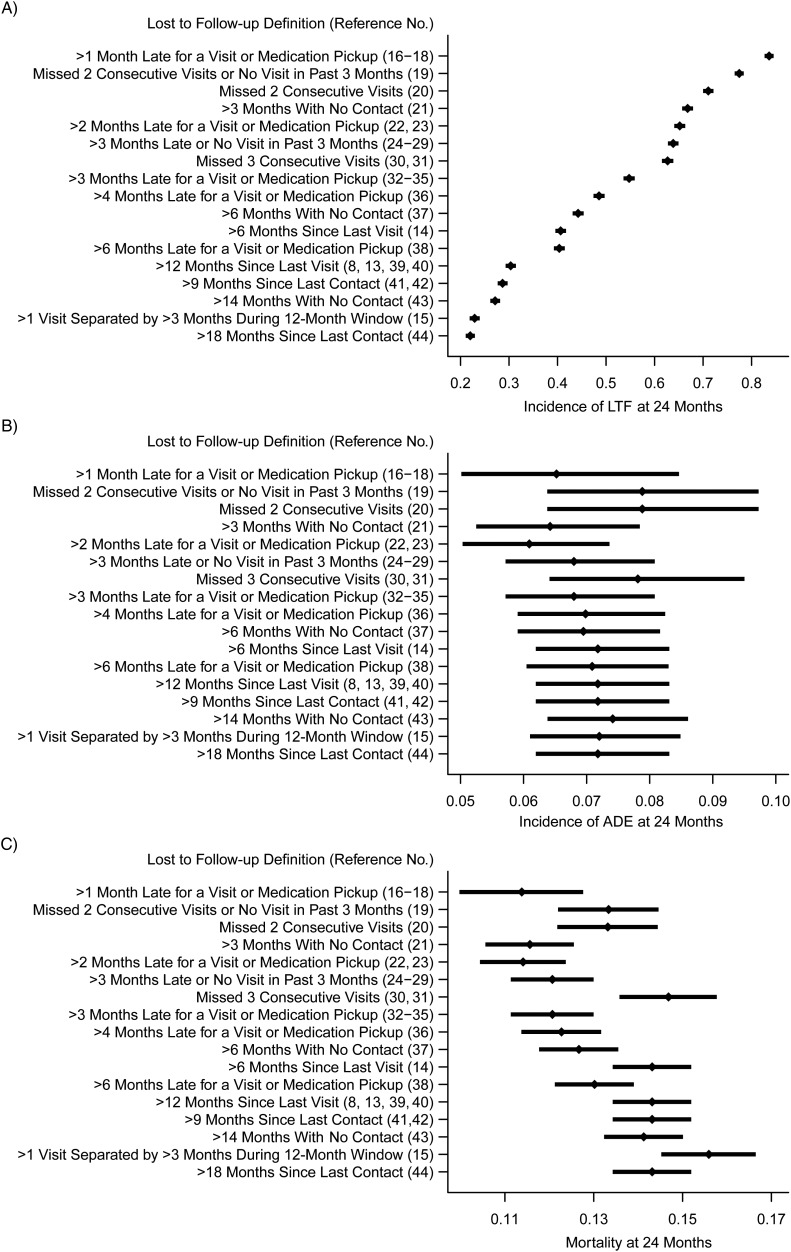
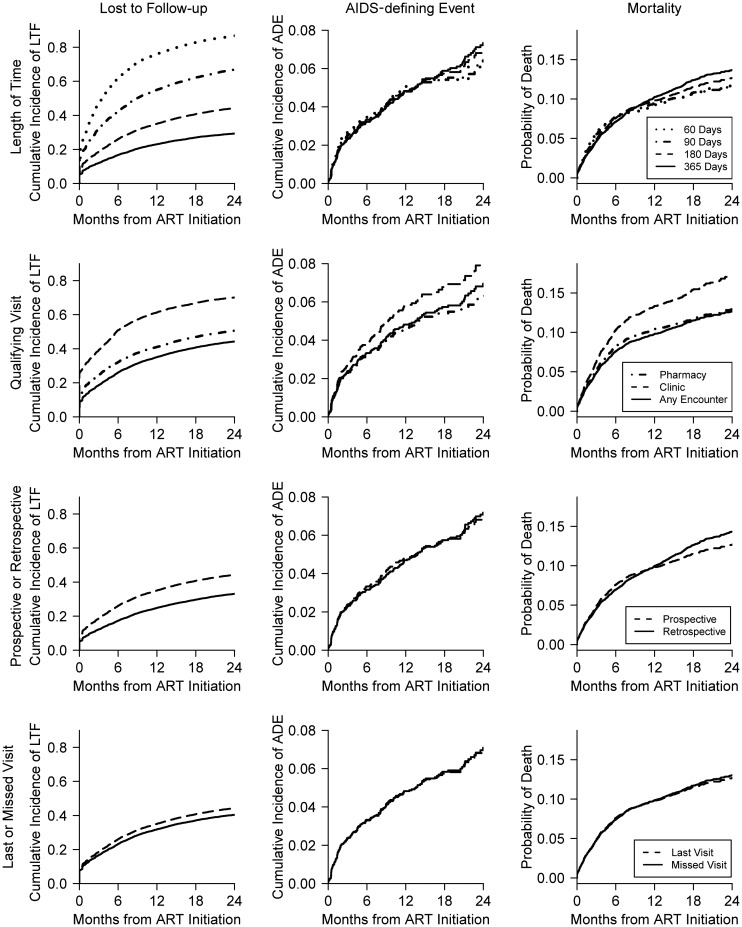
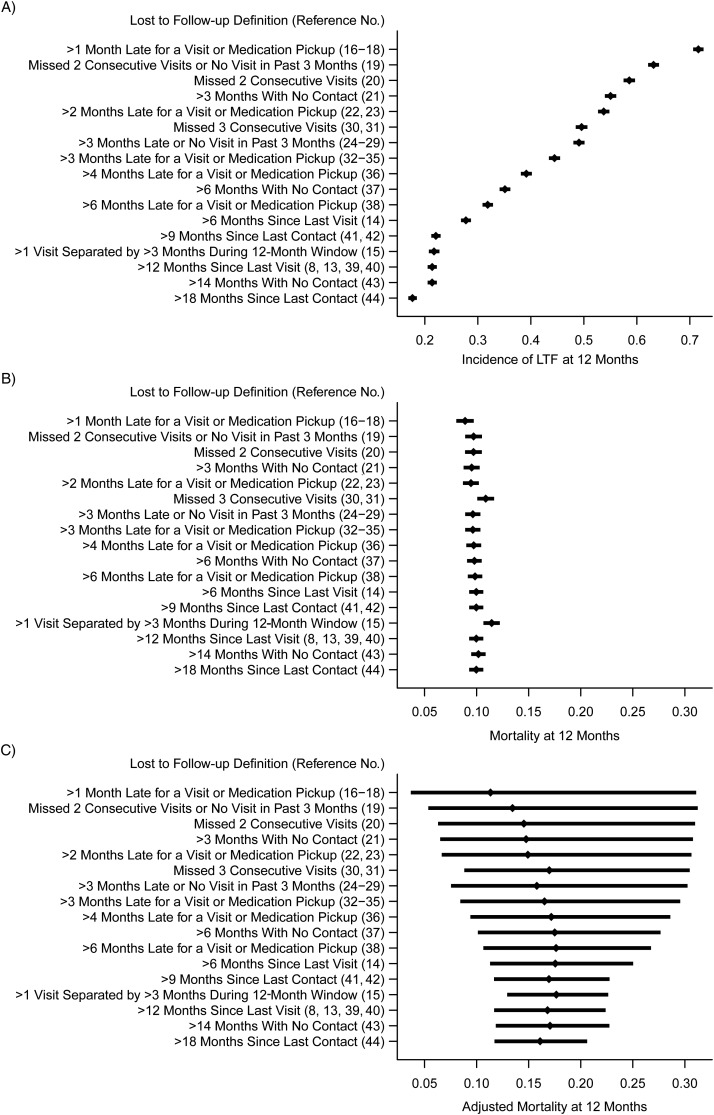
Patient retention is critical to the management of chronic diseases such as human immunodeficiency virus (HIV); hence, accurate measures of loss to follow-up (LTF) are important. Many different LTF definitions have been proposed. In a cohort of 9,692 HIV-infected patients initiating antiretroviral therapy in Mozambique from 2006 to 2011, we investigated the impact of the definition of LTF on estimated rates of LTF, acquired immunodeficiency syndrome (AIDS)-defining events, and death by applying 17 different definitions of LTF gleaned from HIV literature. We further investigated the impact of 4 specific components of the LTF definitions. Cumulative incidences of LTF and AIDS-defining events were estimated by treating death as a competing risk; Kaplan-Meier techniques and variations to account for informative censoring were used to estimate rates of mortality. Estimates of LTF 2 years after treatment initiation were high and varied substantially, from 22% to 84% depending on the LTF definition used. Estimates of 2-year mortality varied from 11% to 16%, and estimates of 2-year AIDS-defining events varied from 6% to 8%. As seen here, the choice of LTF definition can greatly affect study conclusions and program evaluations. Selection of LTF definitions should be based on the study outcome, available data on clinical encounters, and the patients' visit schedules; we suggest some general guidelines.
Keywords: HIV; chronic disease; cohort studies; long-term care; lost to follow-up; program evaluation.
Figures
References
-
- Department of Chronic Diseases and Health Promotion. Preventing Chronic Diseases: A Vital Investment. Geneva, Switzerland: World Health Organization; 2005.
-
- Beaglehole R, Epping-Jordan J, Patel V, et al. Improving the prevention and management of chronic disease in low-income and middle-income countries: a priority for primary health care. Lancet. 2008;372(9642):940–949. - PubMed
-
- Harries AD, Zachariah R, Kapur A, et al. The vital signs of chronic disease management. Trans R Soc Trop Med Hyg. 2009;103(6):537–540. - PubMed
-
- Montaner JS, Hogg R, Wood E, et al. The case for expanding access to highly active antiretroviral therapy to curb the growth of the HIV epidemic. Lancet. 2006;368(9534):531–536. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
