

A UK national audit of hereditary and acquired angioedema
- PMID: 23786259
- PMCID: PMC3898555
- DOI: 10.1111/cei.12159
A UK national audit of hereditary and acquired angioedema
Abstract
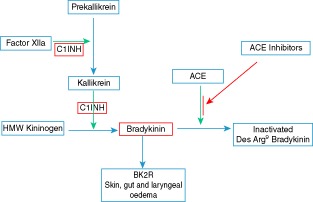
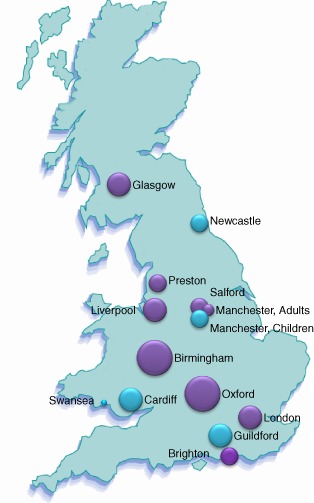
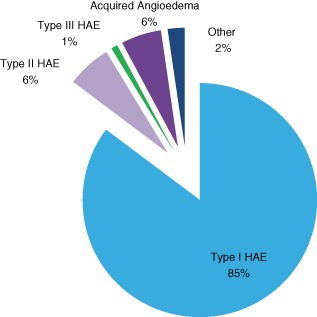
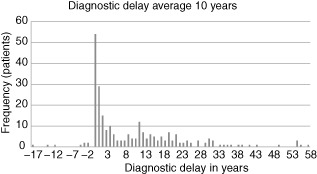
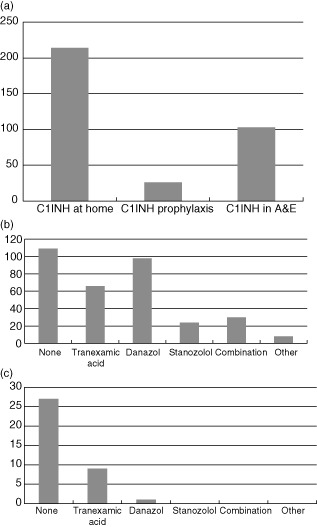
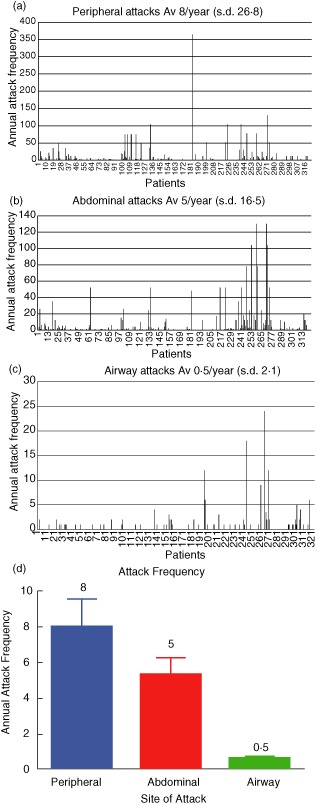
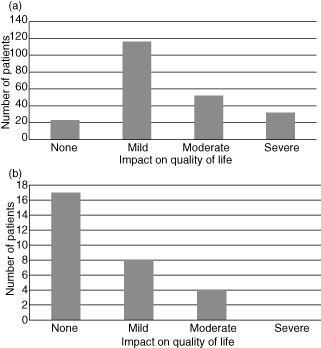
Hereditary angioedema (HAE) and acquired angioedema (AAE) are rare life-threatening conditions caused by deficiency of C1 inhibitor (C1INH). Both are characterized by recurrent unpredictable episodes of mucosal swelling involving three main areas: the skin, gastrointestinal tract and larynx. Swelling in the gastrointestinal tract results in abdominal pain and vomiting, while swelling in the larynx may be fatal. There are limited UK data on these patients to help improve practice and understand more clearly the burden of disease. An audit tool was designed, informed by the published UK consensus document and clinical practice, and sent to clinicians involved in the care of HAE patients through a number of national organizations. Data sets on 376 patients were received from 14 centres in England, Scotland and Wales. There were 55 deaths from HAE in 33 families, emphasizing the potentially lethal nature of this disease. These data also show that there is a significant diagnostic delay of on average 10 years for type I HAE, 18 years for type II HAE and 5 years for AAE. For HAE the average annual frequency of swellings per patient affecting the periphery was eight, abdomen 5 and airway 0·5, with wide individual variation. The impact on quality of life was rated as moderate or severe by 37% of adult patients. The audit has helped to define the burden of disease in the UK and has aided planning new treatments for UK patients.
Keywords: C1 esterase inhibitor, complement; SERPING1; acquired angioedema; hereditary angioedema; primary immunodeficiency; secondary immunodeficiency.
© 2013 British Society for Immunology.
Figures
References
-
- Rosen FS, Pensky J, Donaldson V, Charache P. Hereditary angioneurotic edema: two genetic variants. Science. 1965;148:957–958. - PubMed
-
- Bork K, Barnstedt SE, Koch P, Traupe H. Hereditary angioedema with normal C1-inhibitor activity in women. Lancet. 2000;356:213–217. - PubMed
-
- Zuraw BL, Bork K, E Binkley K, et al. Hereditary angioedema with normal C1 inhibitor function: consensus of an international expert panel. Allergy Asthma Proc. 2012 - PubMed
-
- Cicardi M, Zanichelli A. The acquired deficiency of C1-inhibitor: lymphoproliferation and angioedema. Curr Mol Med. 2010;10:354–360. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
