

Post-extubation dysphagia is associated with longer hospitalization in survivors of critical illness with neurologic impairment
- PMID: 23786755
- PMCID: PMC4057203
- DOI: 10.1186/cc12791
Post-extubation dysphagia is associated with longer hospitalization in survivors of critical illness with neurologic impairment
Abstract
Introduction: Critically ill patients can develop acute respiratory failure requiring endotracheal intubation. Swallowing dysfunction after liberation from mechanical ventilation, also known as post-extubation dysphagia, is common and deleterious among patients without neurologic disease. However, the risk factors associated with the development of post-extubation dysphagia and its effect on hospital lengthofstay in critically ill patients with neurologic disorders remains relatively unexplored.
Methods: We conducted a retrospective, observational cohort study from 2008 to 2010 of patients with neurologic impairment who required mechanical ventilation and subsequently received a bedside swallow evaluation (BSE) by a speech-language pathologist.
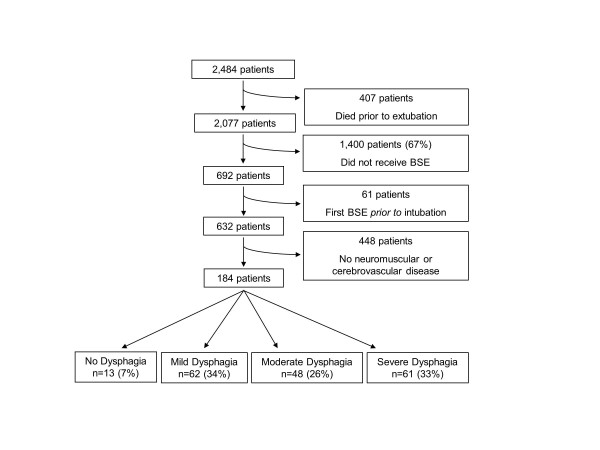
Results: A BSE was performed after mechanical ventilation in 25% (630/2,484) of all patients. In the 184 patients with neurologic impairment, post-extubation dysphagia was present in 93% (171/184), and was classified as mild, moderate, or severe in 34% (62/184), 26% (48/184), and 33% (61/184), respectively. In univariate analyses, statistically significant risk factors for moderate/severe dysphagia included longer durations of mechanical ventilation and the presence of a tracheostomy. In multivariate analysis, adjusting for age, tracheostomy, cerebrovascular disease, and severity of illness, mechanical ventilation for >7 days remained independently associated with moderate/severe dysphagia (adjusted odds ratio=4.48 (95%confidence interval=2.14 to 9.81), P<0.01). The presence of moderate/severe dysphagia was also significantly associated with prolonged hospital lengthofstay, discharge status, and surgical placement of feeding tubes. When adjusting for age, severity of illness, and tracheostomy, patients with moderate/severe dysphagia stayed in the hospital 4.32 days longer after their initial BSE than patients with none/mild dysphagia (95% confidence interval=3.04 to 5.60 days, P<0.01).
Conclusion: In a cohort of critically ill patients with neurologic impairment, longer duration of mechanical ventilation is independently associated with post-extubation dysphagia, and the development of post-extubation dysphagia is independently associated with a longer hospital length of stay after the initial BSE.
Figures
Comment in
-
Neuromuscular disease and extubation dysphagia.Crit Care. 2013 Oct 8;17(5):194. doi: 10.1186/cc12762. Crit Care. 2013. PMID: 24099408 Free PMC article.
Similar articles
-
Neuromuscular disease and extubation dysphagia.Crit Care. 2013 Oct 8;17(5):194. doi: 10.1186/cc12762. Crit Care. 2013. PMID: 24099408 Free PMC article.
-
Postextubation dysphagia is persistent and associated with poor outcomes in survivors of critical illness.Crit Care. 2011;15(5):R231. doi: 10.1186/cc10472. Epub 2011 Sep 29. Crit Care. 2011. PMID: 21958475 Free PMC article.
-
Incidence and factors associated with dysphagia in intensive care unit patients 24 h after extubation.Nurs Crit Care. 2024 Nov;29(6):1479-1488. doi: 10.1111/nicc.13026. Epub 2024 Mar 1. Nurs Crit Care. 2024. PMID: 38429877
-
Post-extubation dysphagia incidence in critically ill patients: A systematic review and meta-analysis.Aust Crit Care. 2021 Jan;34(1):67-75. doi: 10.1016/j.aucc.2020.05.008. Epub 2020 Jul 29. Aust Crit Care. 2021. PMID: 32739246
-
Ventilatory support after extubation in critically ill patients.Lancet Respir Med. 2018 Dec;6(12):948-962. doi: 10.1016/S2213-2600(18)30375-8. Lancet Respir Med. 2018. PMID: 30629933 Review.
Cited by
-
Neuromuscular disease and extubation dysphagia.Crit Care. 2013 Oct 8;17(5):194. doi: 10.1186/cc12762. Crit Care. 2013. PMID: 24099408 Free PMC article.
-
Interventions to enable communication for adult patients requiring an artificial airway with or without mechanical ventilator support.Cochrane Database Syst Rev. 2021 Oct 12;10(10):CD013379. doi: 10.1002/14651858.CD013379.pub2. Cochrane Database Syst Rev. 2021. PMID: 34637143 Free PMC article.
-
Persistent swallowing disorders after extubation in mechanically ventilated patients in ICU: a two-center prospective study.Ann Intensive Care. 2020 Oct 14;10(1):138. doi: 10.1186/s13613-020-00752-x. Ann Intensive Care. 2020. PMID: 33052476 Free PMC article.
-
Patients with dysphagia: How to supply nutrition through non-tube feeding.Front Nutr. 2022 Dec 2;9:1060630. doi: 10.3389/fnut.2022.1060630. eCollection 2022. Front Nutr. 2022. PMID: 36532550 Free PMC article. Review.
-
Pharyngolaryngeal Sensory Deficits in Patients with Middle Cerebral Artery Infarction: Lateralization and Relation to Overall Dysphagia Severity.Cerebrovasc Dis Extra. 2017;7(3):130-139. doi: 10.1159/000479483. Epub 2017 Oct 3. Cerebrovasc Dis Extra. 2017. PMID: 28972945 Free PMC article.
References
-
- Suarez JI, Zaidat OO, Suri MF, Feen ES, Lynch G, Hickman J, Georgiadis A, Selman WR. Length of stay and mortality in neurocritically ill patients: impact of a specialized neurocritical care team. Crit Care Med. 2004;17:2311–2317. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
