

Gender and racial differences in focal and global acetabular version
- PMID: 23786986
- PMCID: PMC4049456
- DOI: 10.1016/j.arth.2013.05.015
Gender and racial differences in focal and global acetabular version
Abstract
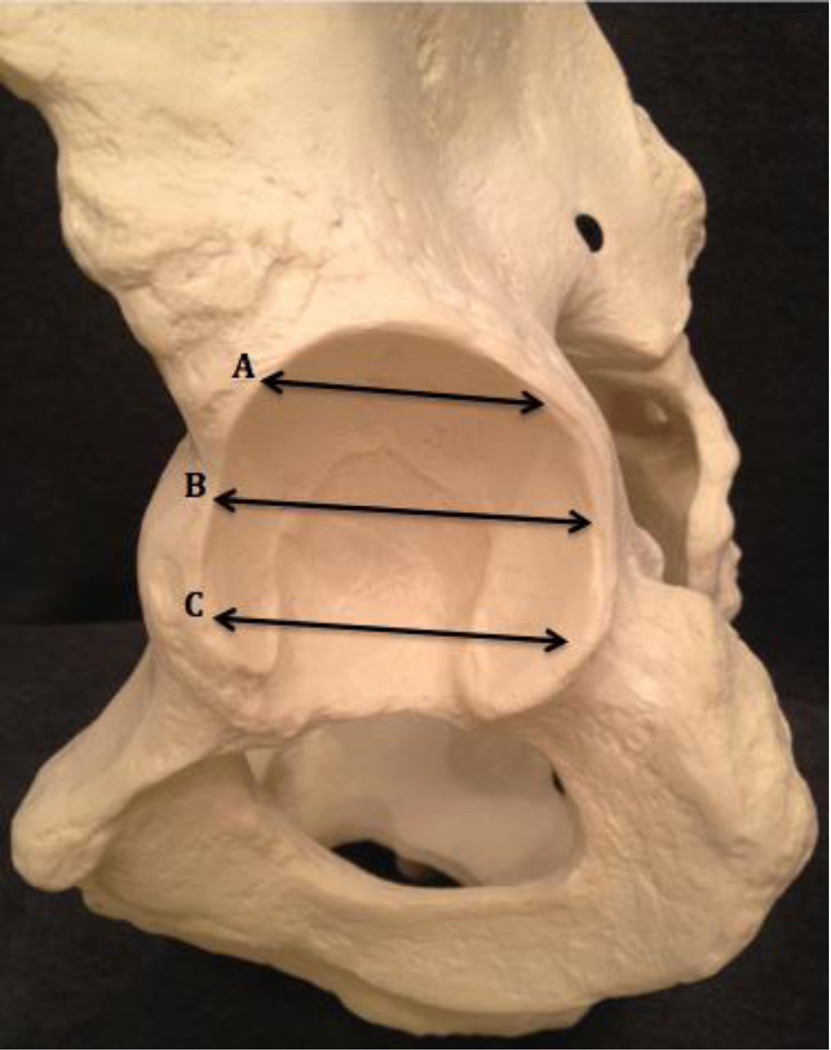
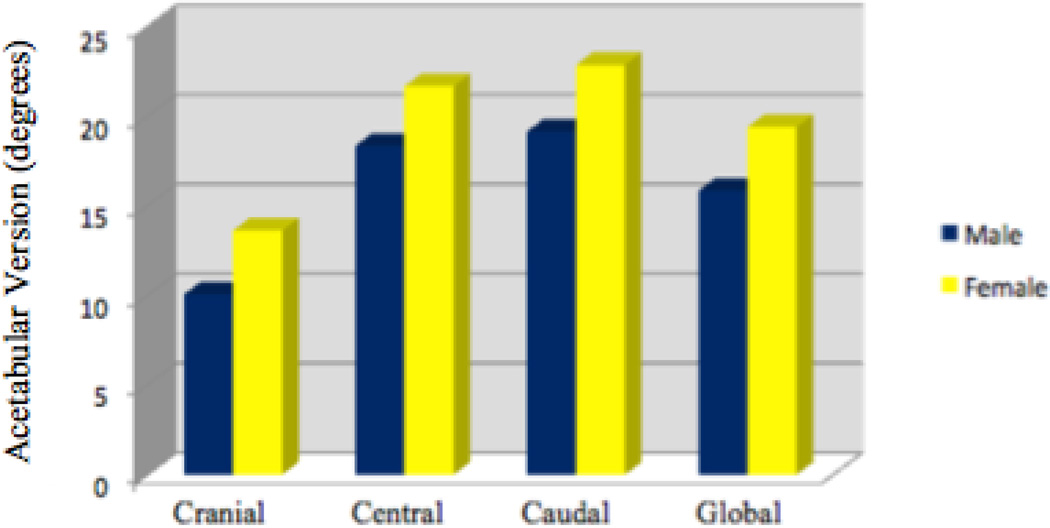
The purpose of this study was to compare the acetabular version between male and female pelvises. We hypothesized that female acetabula would demonstrate more retroversion because Pincer-type femoroacetabular impingement (FAI) is associated with acetabular retroversion, which is more commonly observed in females. 120 bony pelvic specimens were randomly collected. The version was measured at three different axial sections of each acetabulum: cranial, central, and caudal. Males demonstrated significantly less anteversion than females in every section. The global version (the average of all three measurements) was also significantly different between males and females (16° ± 7° and 19° ± 8° respectively, P<0.001). Of the 240 examined acetabuli, 21 demonstrated cranial retroversion (16 males & 5 females). The data showed no significant difference (P=0.353) between global version of African Americans (18° ± 9°) and Caucasians (17° ± 7°). The results of this study suggest that symptomatic FAI in the female population likely reflects a complex interplay of femoral and acetabular dysmorphology and cannot be explained by differences in acetabular version alone.
Keywords: acetabular retroversion; femoroacetabular impingement; hip impingement; hip pain; pincer impingement.
Copyright © 2014 Elsevier Inc. All rights reserved.
Figures

References
-
- Dandachli W, Islam SU, Liu M, et al. Three-dimensional CT analysis to determine acetabular retroversion and the implications for the management of femoro-acetabular impingement. J Bone Joint Surg Br. 2009;91(8):1031. - PubMed
-
- Beck M, Leunig M, Parvizi J, et al. Anterior femoroacetabular impingement: part II. Midterm results of surgical treatment. Clin Orthop Relat Res. 2004;(418):67. - PubMed
-
- Ganz R, Parvizi J, Beck M, et al. Femoroacetabular impingement: a cause for osteoarthritis of the hip. Clin Orthop Relat Res. 2003;(417):112. - PubMed
-
- Murphy S, Tannast M, Kim YJ, et al. Debridement of the adult hip for femoroacetabular impingement: indications and preliminary clinical results. Clin Orthop Relat Res. 2004;(429):178. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
