

The urine output definition of acute kidney injury is too liberal
- PMID: 23787055
- PMCID: PMC4056349
- DOI: 10.1186/cc12784
The urine output definition of acute kidney injury is too liberal
Abstract
Introduction: The urine output criterion of 0.5 ml/kg/hour for 6 hours for acute kidney injury (AKI) has not been prospectively validated. Urine output criteria for AKI (AKIUO) as predictors of in-hospital mortality or dialysis need were compared.
Methods: All admissions to a general ICU were prospectively screened for 12 months and hourly urine output analysed in collection intervals between 1 and 12 hours. Prediction of the composite of mortality or dialysis by urine output was analysed in increments of 0.1 ml/kg/hour from 0.1 to 1 ml/kg/hour and the optimal threshold for each collection interval determined. AKICr was defined as an increase in plasma creatinine≥26.5 μmol/l within 48 hours or ≥50% from baseline.
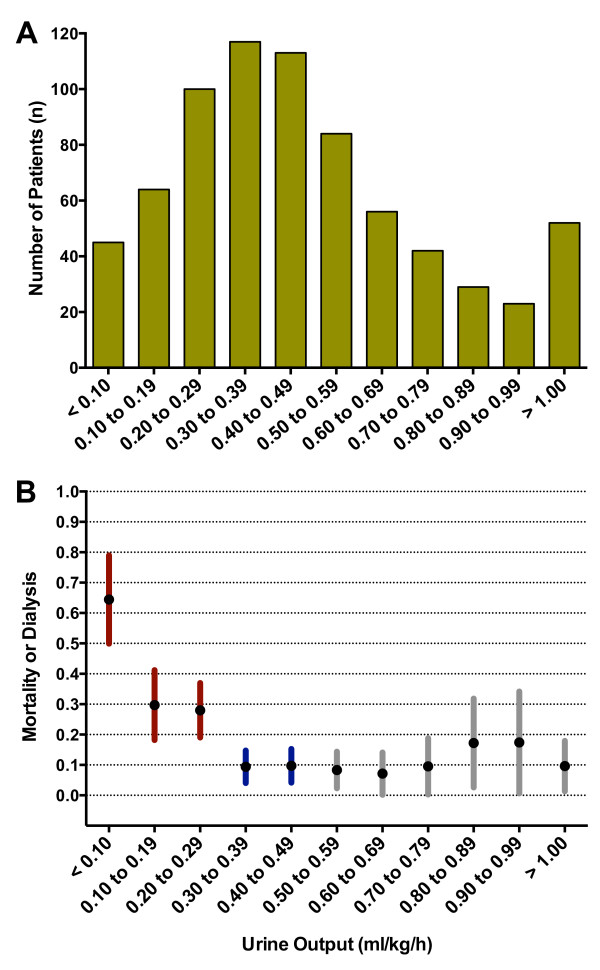
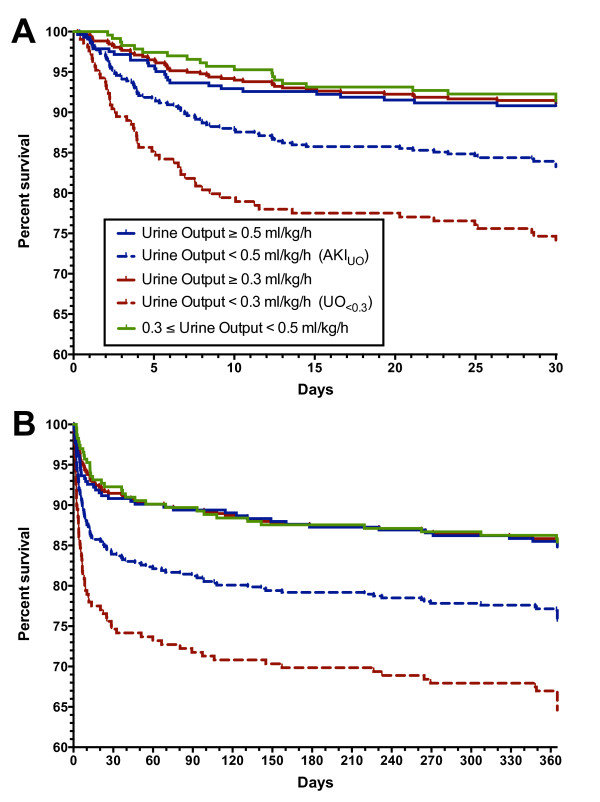
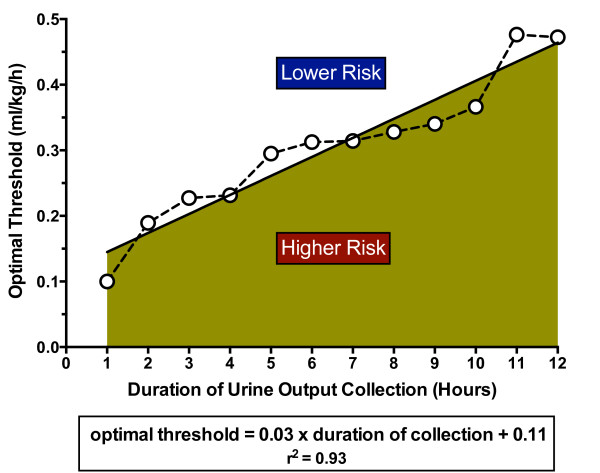
Results: Of 725 admissions, 72% had either AKICr or AKIUO or both. AKIUO (33.7%) alone was more frequent than AKICr (11.0%) alone (P<0.0001). A 6-hour urine output collection threshold of 0.3 ml/kg/hour was associated with a stepped increase in in-hospital mortality or dialysis (from 10% above to 30% less than 0.3 ml/kg/hour). Hazard ratios for in-hospital mortality and 1-year mortality were 2.25 (1.40 to 3.61) and 2.15 (1.47 to 3.15) respectively after adjustment for age, body weight, severity of illness, fluid balance, and vasopressor use. In contrast, after adjustment AKIUO was not associated with in-hospital mortality or 1-year mortality. The optimal urine output threshold was linearly related to duration of urine collection (r2=0.93).
Conclusions: A 6-hour urine output threshold of 0.3 ml/kg/hour best associated with mortality and dialysis, and was independently predictive of both hospital mortality and 1-year mortality. This suggests that the current AKI urine output definition is too liberally defined. Shorter urine collection intervals may be used to define AKI using lower urine output thresholds.
Figures
References
-
- Bellomo R, Ronco C, Kellum JA, Mehta RL, Palevsky PM. Acute Dialysis Quality Initiative Workgroup. Acute renal failure - definition, outcome measures, animal models, fluid therapy and information technology needs: the Second International Consensus Conference of the Acute Dialysis Quality Initiative (ADQI) Group. Crit Care. 2004;17:R204–R412. doi: 10.1186/cc2872. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
