

Groove pancreatitis: spectrum of imaging findings and radiology-pathology correlation
- PMID: 23789694
- PMCID: PMC4005339
- DOI: 10.2214/AJR.12.9956
Groove pancreatitis: spectrum of imaging findings and radiology-pathology correlation
Abstract
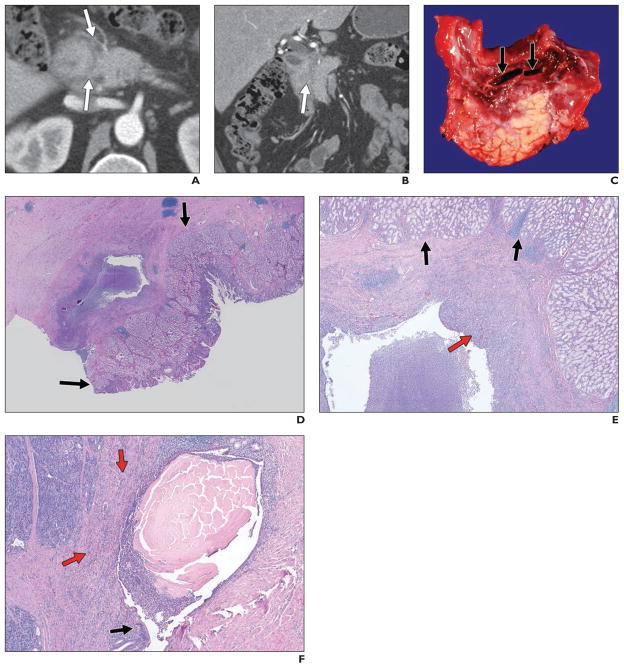
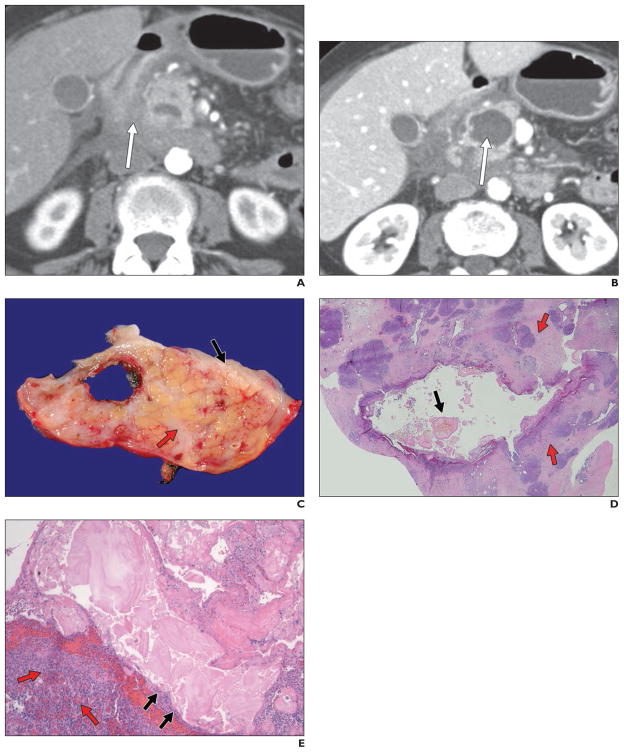
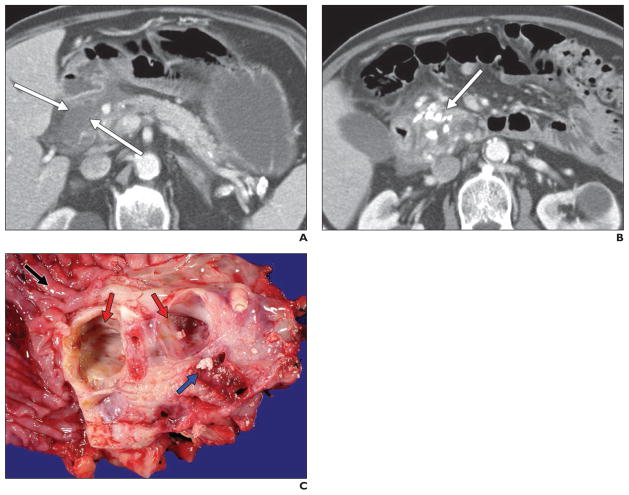
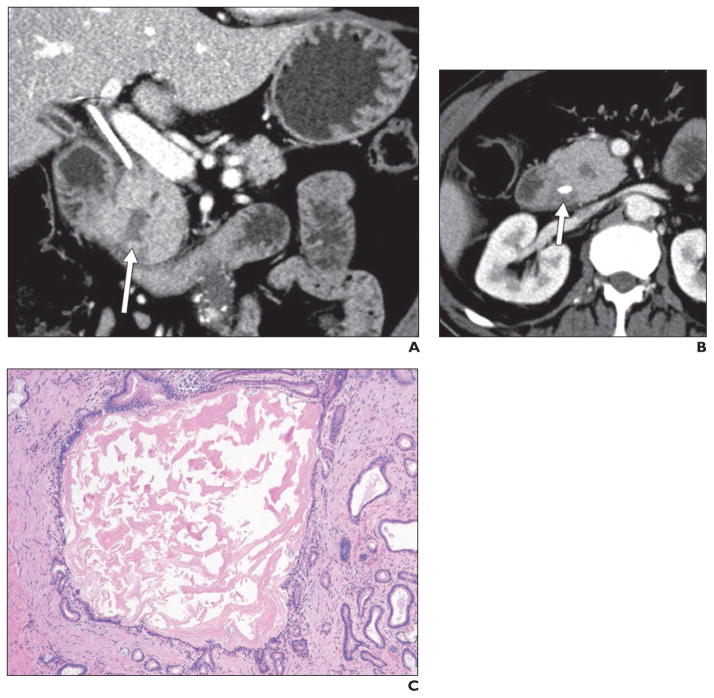
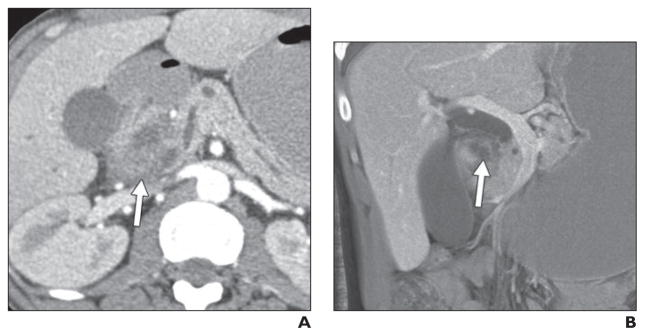
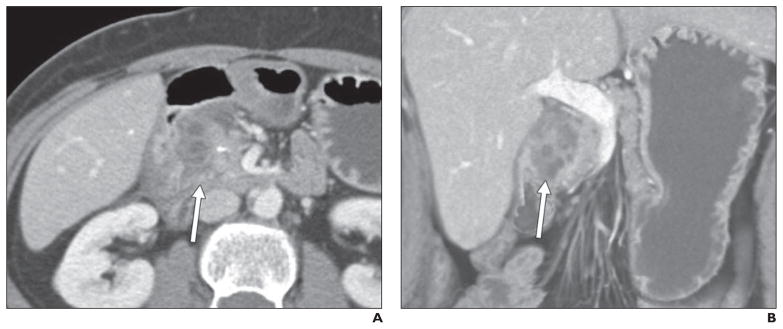
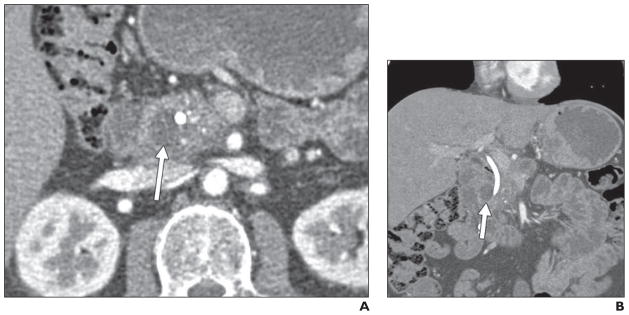
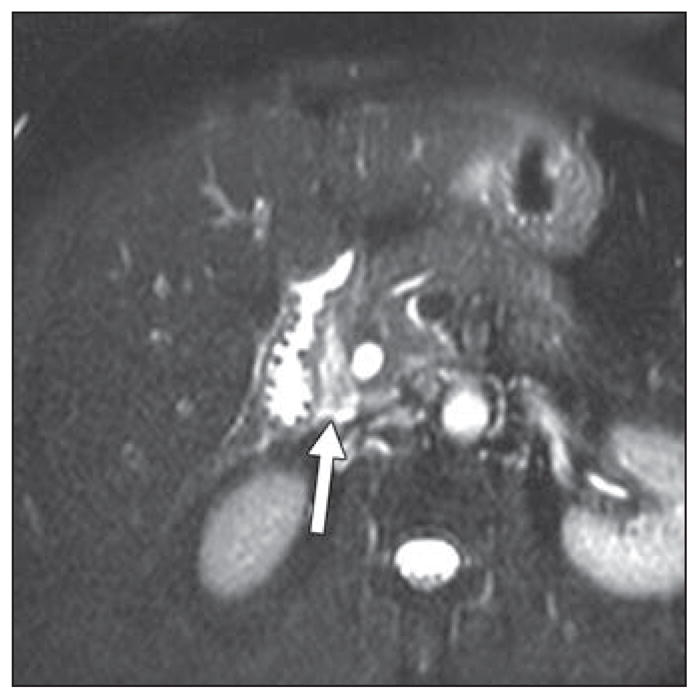
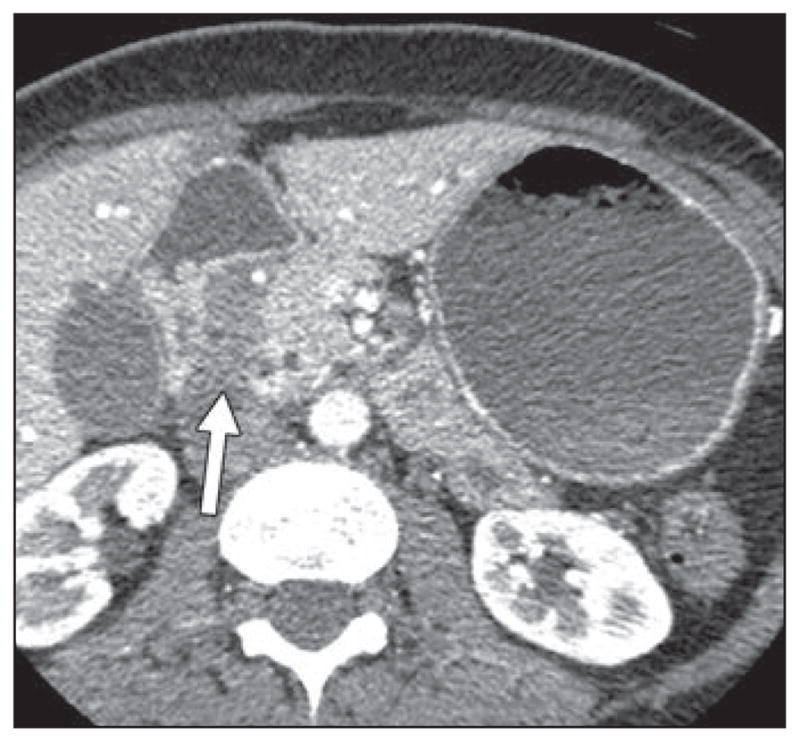
Objective: Groove pancreatitis is a rare form of chronic pancreatitis affecting the "groove" between the pancreatic head, duodenum, and common bile duct. The exact cause is unknown, although there are strong associations with long-term alcohol abuse, functional obstruction of the duct of Santorini, and Brunner gland hyperplasia.
Conclusion: Unfortunately, differentiating groove pancreatitis from malignancy on the basis of imaging features, clinical presentation, or laboratory markers can be extraordinarily difficult, and the vast majority of these patients ultimately undergo a pancreaticoduodenectomy (Whipple procedure) because of an inability to completely exclude malignancy. In certain cases, however, the imaging features on CT and MRI can allow the radiologist to prospectively suggest the correct diagnosis.
Figures

References
-
- Becker V. Bauchspeicheldruse (Inselapperat ausgenommen) In: Doerr W, editor. Spezielle pathologische anatomie. Berlin, Germany: Springer-Verlag; 1973.
-
- Blasbalg R, Baroni RH, Costa DN, et al. MRI features of groove pancreatitis. AJR. 2007;189:73–80. - PubMed
-
- Balakrishnan V, Chatni S, Radhakirshnan L, et al. Groove pancreatitis: a case report and review of the literature. JOP. 2007;8:592–597. - PubMed
-
- Triantopoulou C, Dervenis C, Giannakou N, et al. Groove pancreatitis: a diagnostic challenge. Eur Radiol. 2009;19:1736–1743. - PubMed
-
- Tezuka K, Makino TY, Hirai I, Kimura W. Groove pancreatitis. Dig Surg. 2010;27:149–152. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
