

Predicting right ventricular failure in the modern, continuous flow left ventricular assist device era
- PMID: 23791165
- PMCID: PMC4111251
- DOI: 10.1016/j.athoracsur.2013.03.099
Predicting right ventricular failure in the modern, continuous flow left ventricular assist device era
Abstract
Background: In the era of destination continuous flow left ventricular assist devices (LVAD), the decision of whether a patient will tolerate isolated LVAD support or will need biventricular support (BIVAD) can be challenging. Incorrect decision making with delayed right ventricular (RV) assist device implantation results in increased morbidity and mortality. Continuous flow LVADs have been shown to decrease pulmonary hypertension and improve RV function. We undertook this study to determine predictors in the continuous flow LVAD era that identify patients who are candidates for isolated LVAD therapy as opposed to biventricular support.
Methods: We reviewed demographic, hemodynamic, laboratory, and echocardiographic variables for 218 patients who underwent VAD implant from 2003 through 2011 (LVAD=167, BIVAD=51), during the era of continuous flow LVADs.
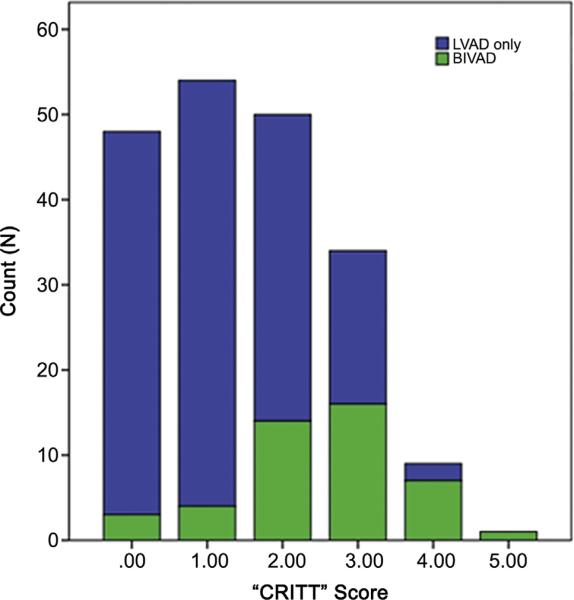
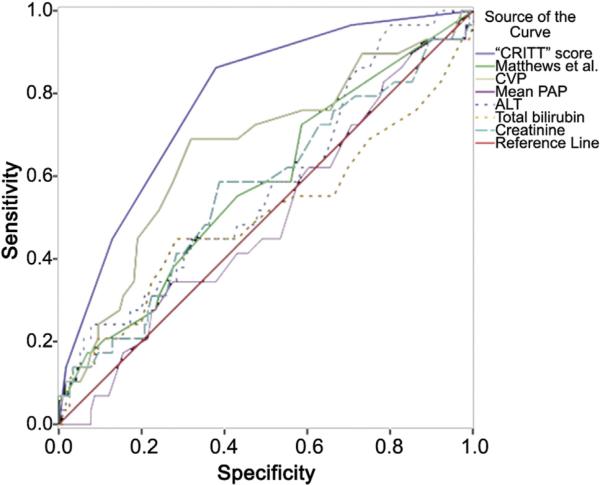
Results: Fifty preoperative risk factors were compared between patients who were successfully managed with an LVAD and those who required a BIVAD. Seventeen variables demonstrated statistical significance by univariate analysis. Multivariable logistic regression analysis identified central venous pressure>15 mmHg (OR 2.0, "C"), severe RV dysfunction (OR 3.7, "R"), preoperative intubation (OR 4.3, "I"), severe tricuspid regurgitation (OR 4.1, "T"), heart rate>100 (OR 2.0, Tachycardia-"T")-CRITT as the major criteria predictive of the need for biventricular support. Utilizing these data, a highly sensitive and easy to use risk score for determining RV failure was generated that outperformed other established risk stratification tools.
Conclusions: We present a preoperative risk calculator to determine suitability of a patient for isolated LVAD support in the current continuous flow ventricular assist device era.
Keywords: 27.
Copyright © 2013 The Society of Thoracic Surgeons. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Rose EA, Gelijns AC, Moskowitz AJ, et al. Long-term use of a left ventricular assist device for end-stage heart failure. N Engl J Med. 2001;345:1435–43. - PubMed
-
- Miller LW, Pagani FD, Russell SD, et al. Use of a continuous-flow device in patients awaiting heart transplantation. N Engl J Med. 2007;357:885–96. - PubMed
-
- Slaughter MS, Rogers JG, Milano CA, et al. Advanced heart failure treated with continuous-flow left ventricular assist device. N Engl J Med. 2009;361:2241–51. - PubMed
-
- Rogers JG, Aaronson KD, Boyle AJ, et al. Continuous flow left ventricular assist device improves functional capacity and quality of life of advanced heart failure patients. J Am Coll Cardiol. 2010;55:1826–34. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
