

The impact of maximum rectal distention and tandem angle on rectal dose delivered in 3D planned gynecologic high dose-rate brachytherapy
- PMID: 23792603
- PMCID: PMC3706279
- DOI: 10.1097/IGC.0b013e3182959030
The impact of maximum rectal distention and tandem angle on rectal dose delivered in 3D planned gynecologic high dose-rate brachytherapy
Abstract
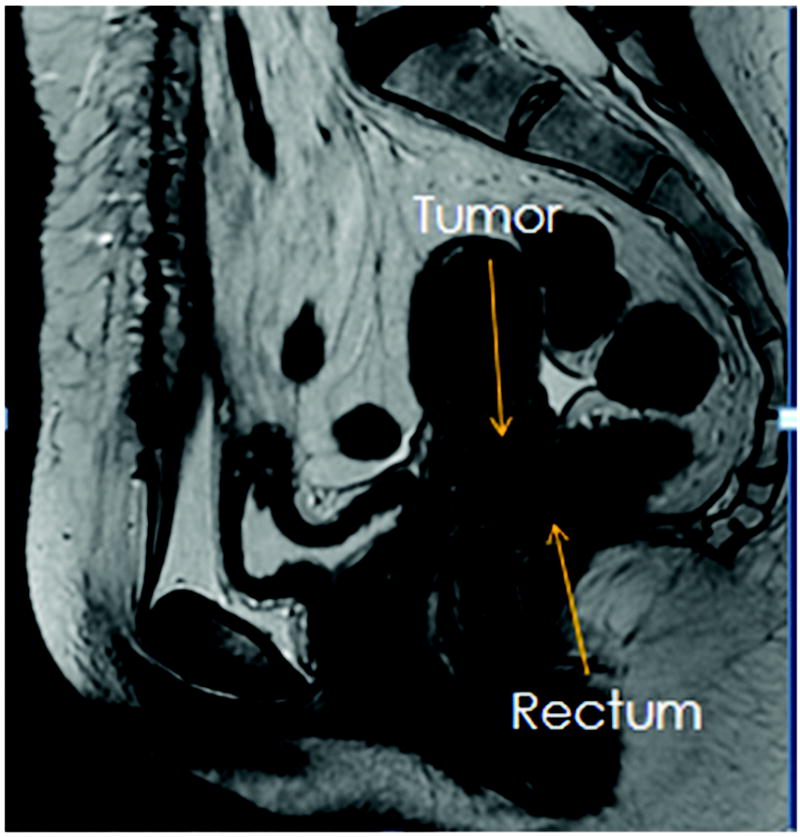
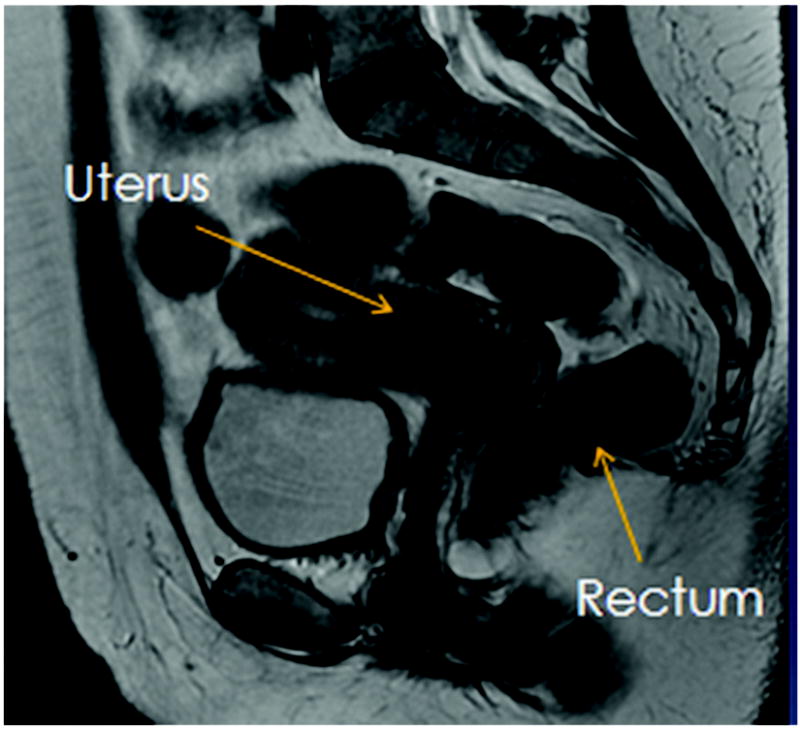
Objective: Computed tomography-based treatment planning for cervical cancer has allowed investigation into the volumetric radiation dose delivered to the rectum. The goal of intracavitary brachytherapy is to maximize the tumor dose while decreasing the dose to normal tissue like the rectum. We investigated the effects of tandem angle and maximum rectal distention on rectal dose delivered in HDR brachytherapy for locally advanced cervical cancer.
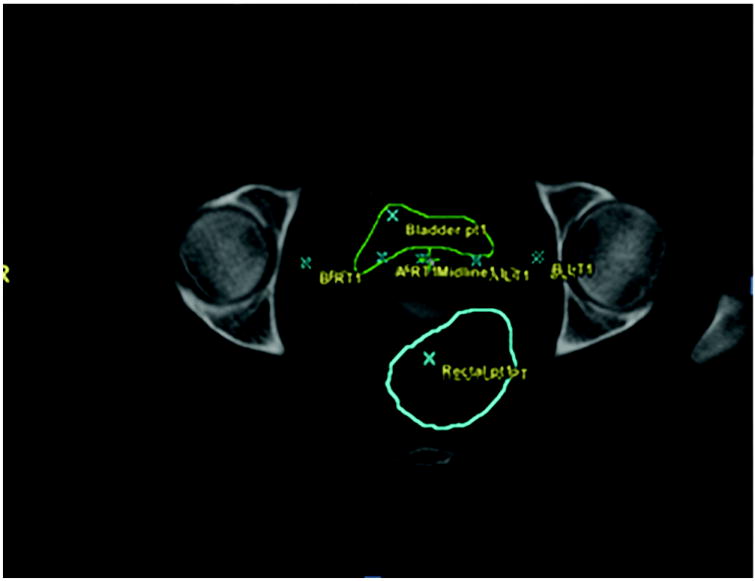
Materials and methods: Between July 2007 and January 2010, 97 brachytherapy treatment planning computed tomographic scans from the first and last implant of 51 patients with locally advanced cervical cancer were reviewed. The rectum was manually contoured from the ischial tuberosity to the bottom of the sacroiliac joint. The maximum rectal distention was determined by measuring the largest anterior-posterior diameter of the rectum superior to the tandem ring and inferior to the end of the applicator. A volumetric measurement of the maximum and mean rectal dose, dose to 2 cc (D2cc), dose to 1cc (D1cc) of the rectum was calculated. The tandem angle and the Internal Commission on Radiation Units and Measurement rectal point were recorded, and a dose volume histogram was referenced.
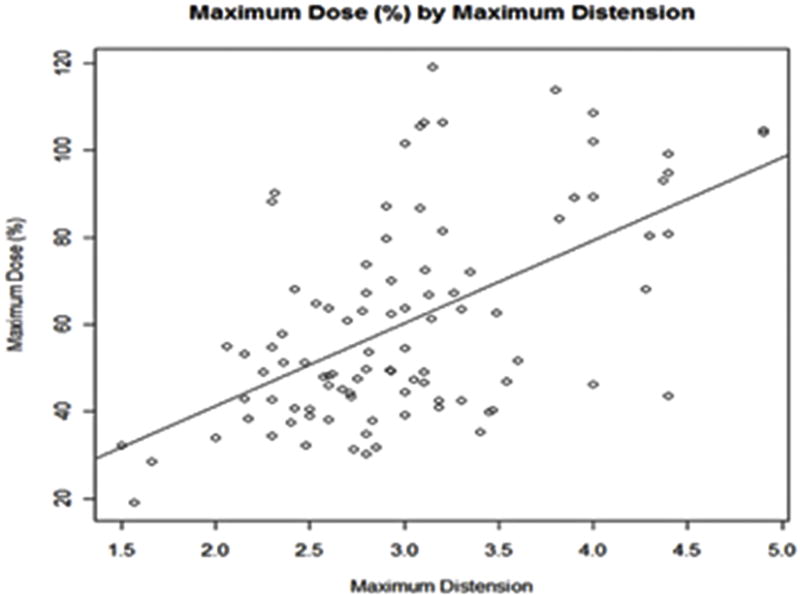
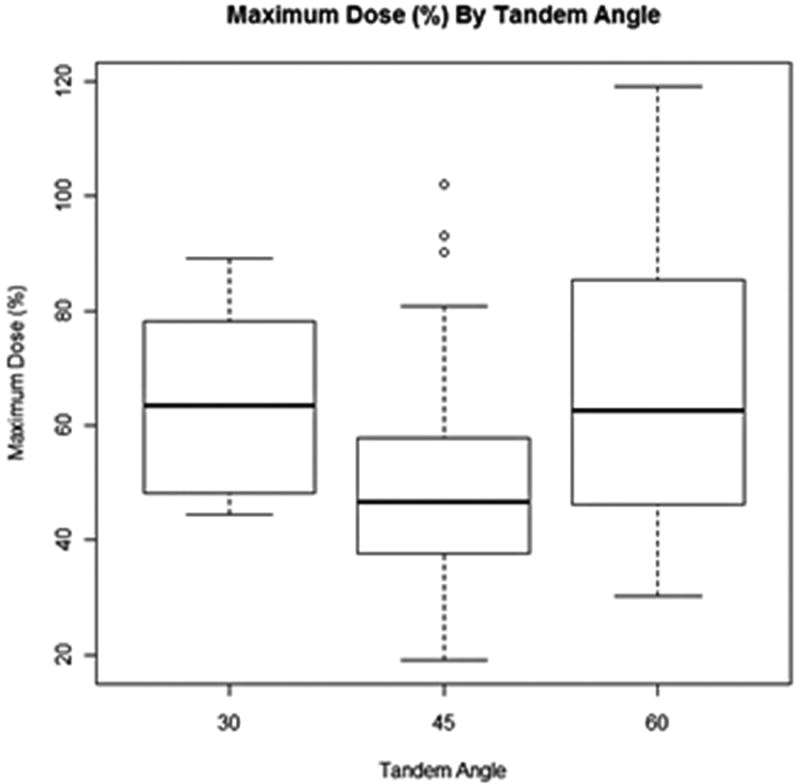
Results: The mean maximum rectal distention was 3.01 cm. The mean D1cc, D2cc, mean rectal dose, maximum rectal dose, and Internal Commission on Radiation Units and Measurement rectal dose were 3.03 Gy, 2.78 Gy, 4.19 cGy, 1.40 cGy, and 2.99 Gy per treatment, respectively. In a multivariate analysis controlling for surface area, tandem angle, and body mass index, there was a significant increase in D2cc with increasing rectal distention (P = 0.016). There were no significant findings when observing the effects of tandem angle on D2cc.
Conclusion: Rectal distention significantly affects D2cc delivered in HDR brachytherapy. In contrast, tandem angle does not. Concerted efforts to decrease rectal distention should be considered during treatment planning and delivery.
Figures
References
-
- Haie-Meder C, Morice P, Castiglione M. Cervical cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2010;21(Suppl 5):v37–40. - PubMed
-
- Nag S, Erickson B, Thomadsen B, et al. The American Brachytherapy Society recommendations for high-dose-rate brachytherapy for carcinoma of the cervix. Int J Radiat Oncol Biol Phys. 2000;48:201–211. - PubMed
-
- Gao M, Albuquerque K, Chi A, et al. 3D CT-based volumetric dose assessment of 2D plans using GEC-ESTRO guidelines for cervical cancer brachytherapy. Brachytherapy. 2010;9:55–60. - PubMed
-
- Haie-Meder C, Chargari C, Rey A, et al. DVH parameters and outcome for patients with early-stage cervical cancer treated with preoperative MRI-based low dose rate brachytherapy followed by surgery. Radiother Oncol. 2009;93:316–321. - PubMed
-
- Pelloski CE, Palmer M, Chronowski GM, et al. Comparison between CT-based volumetric calculations and ICRU reference-point estimates of radiation doses delivered to bladder and rectum during intracavitary radiotherapy for cervical cancer. Int J Radiat Oncol Biol Phys. 2005;62:131–137. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
