

Near-infrared fluorescence-guided resection of colorectal liver metastases
- PMID: 23794086
- PMCID: PMC3775857
- DOI: 10.1002/cncr.28203
Near-infrared fluorescence-guided resection of colorectal liver metastases
Abstract
Background: The fundamental principle of oncologic surgery is the complete resection of malignant cells. However, small tumors are often difficult to find during surgery using conventional techniques. The objectives of this study were to determine if optical imaging, using a contrast agent already approved for other indications, could improve hepatic metastasectomy with curative intent, to optimize dose and timing, and to determine the mechanism of contrast agent accumulation.
Methods: The high tissue penetration of near-infrared (NIR) light was exploited by use of the FLARE (Fluorescence-Assisted Resection and Exploration) image-guided surgery system and the NIR fluorophore indocyanine green in a clinical trial of 40 patients undergoing hepatic resection for colorectal cancer metastases.
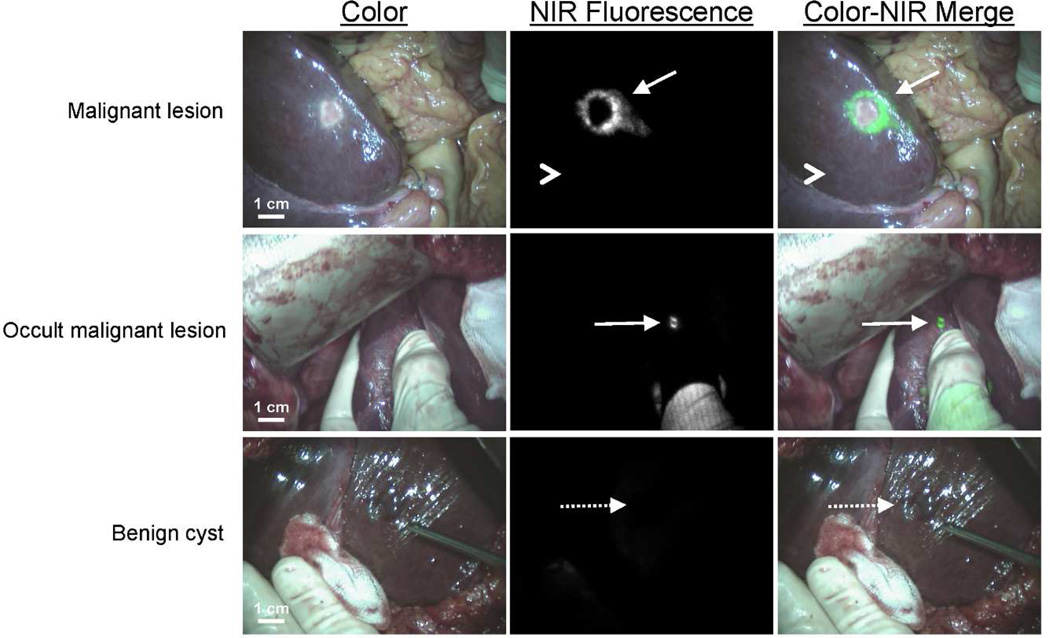
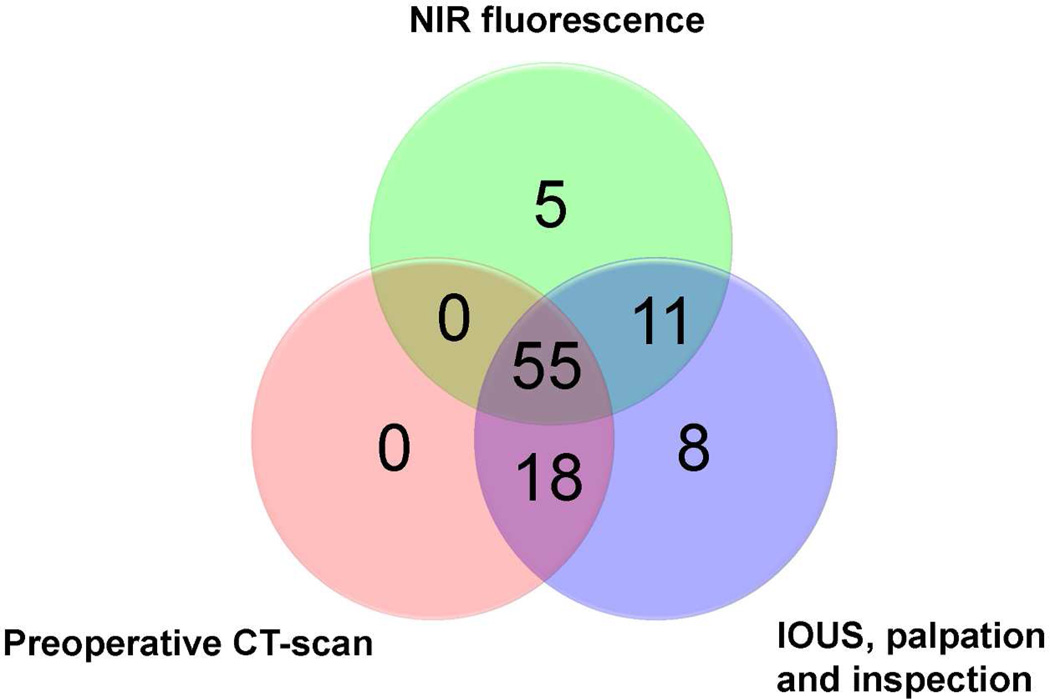
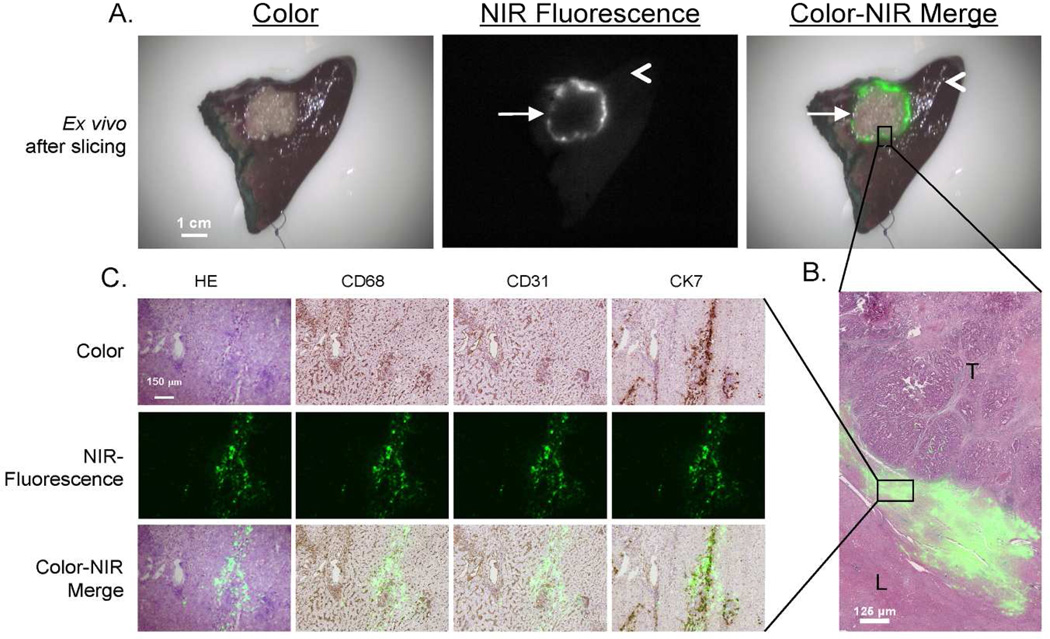
Results: A total of 71 superficially located (< 6.2 mm beneath the liver capsule) colorectal liver metastases were identified and resected using NIR fluorescence imaging. Median tumor-to-liver ratio was 7.0 (range, 1.9-18.7) and no significant differences between time points or doses were found. Indocyanine green fluorescence was seen as a rim around the tumor, which is shown to be entrapment around cytokeratin 7-positive hepatocytes compressed by the tumor. Importantly, in 5 of 40 patients (12.5%, 95% confidence interval = 5.0-26.6), additional small and superficially located lesions were detected using NIR fluorescence, and were otherwise undetectable by preoperative computed tomography, intraoperative ultrasound, visual inspection, and palpation.
Conclusions: NIR fluorescence imaging, even when used with a nontargeted, clinically available NIR fluorophore, is complementary to conventional imaging and able to identify missed lesions by other modalities.
Keywords: colorectal cancer; fluorescence; image-guided surgery; indocyanine green; liver neoplasms; near-infrared.
© 2013 American Cancer Society.
Figures
References
-
- Rees M, Tekkis PP, Welsh FK, O'Rourke T, John TG. Evaluation of long-term survival after hepatic resection for metastatic colorectal cancer: a multifactorial model of 929 patients. Ann Surg. 2008;247:125–135. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
