

Anaemia, prenatal iron use, and risk of adverse pregnancy outcomes: systematic review and meta-analysis
- PMID: 23794316
- PMCID: PMC3689887
- DOI: 10.1136/bmj.f3443
Anaemia, prenatal iron use, and risk of adverse pregnancy outcomes: systematic review and meta-analysis
Abstract
Objectives: To summarise evidence on the associations of maternal anaemia and prenatal iron use with maternal haematological and adverse pregnancy outcomes; and to evaluate potential exposure-response relations of dose of iron, duration of use, and haemoglobin concentration in prenatal period with pregnancy outcomes.
Design: Systematic review and meta-analysis
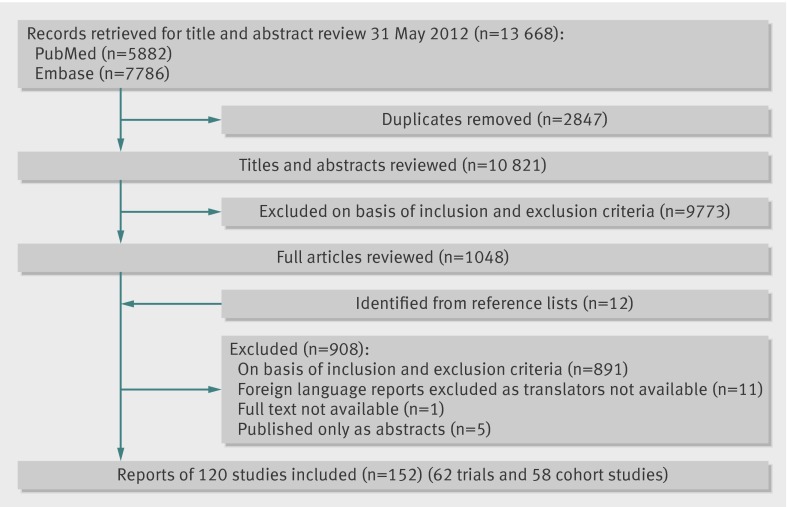
Data sources: Searches of PubMed and Embase for studies published up to May 2012 and references of review articles.
Study selection criteria: Randomised trials of prenatal iron use and prospective cohort studies of prenatal anaemia; cross sectional and case-control studies were excluded.
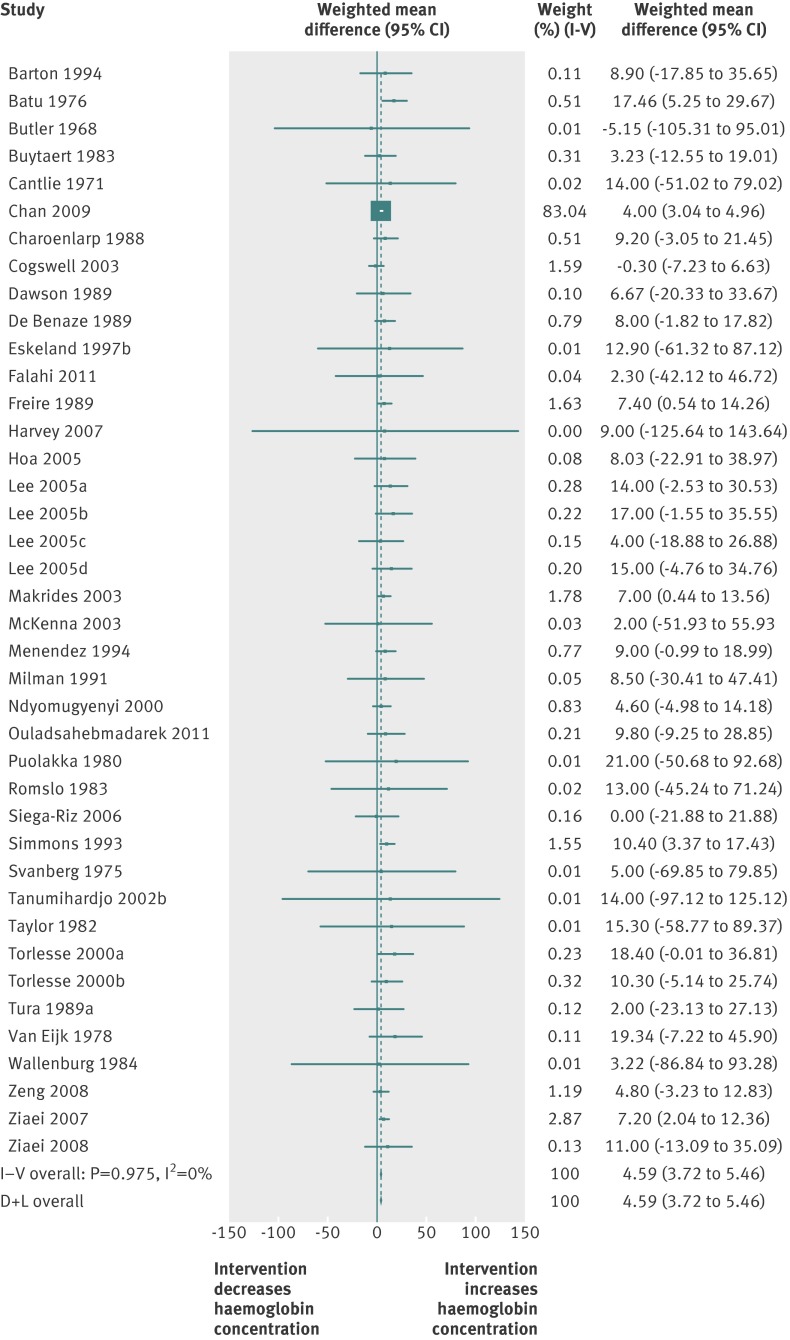
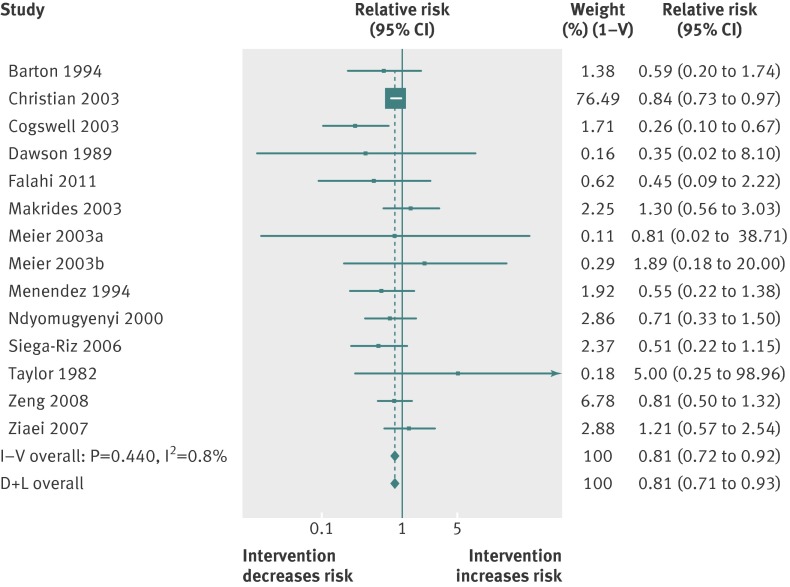
Results: 48 randomised trials (17 793 women) and 44 cohort studies (1 851 682 women) were included. Iron use increased maternal mean haemoglobin concentration by 4.59 (95% confidence interval 3.72 to 5.46) g/L compared with controls and significantly reduced the risk of anaemia (relative risk 0.50, 0.42 to 0.59), iron deficiency (0.59, 0.46 to 0.79), iron deficiency anaemia (0.40, 0.26 to 0.60), and low birth weight (0.81, 0.71 to 0.93). The effect of iron on preterm birth was not significant (relative risk 0.84, 0.68 to 1.03). Analysis of cohort studies showed a significantly higher risk of low birth weight (adjusted odds ratio 1.29, 1.09 to 1.53) and preterm birth (1.21, 1.13 to 1.30) with anaemia in the first or second trimester. Exposure-response analysis indicated that for every 10 mg increase in iron dose/day, up to 66 mg/day, the relative risk of maternal anaemia was 0.88 (0.84 to 0.92) (P for linear trend<0.001). Birth weight increased by 15.1 (6.0 to 24.2) g (P for linear trend=0.005) and risk of low birth weight decreased by 3% (relative risk 0.97, 0.95 to 0.98) for every 10 mg increase in dose/day (P for linear trend<0.001). Duration of use was not significantly associated with the outcomes after adjustment for dose. Furthermore, for each 1 g/L increase in mean haemoglobin, birth weight increased by 14.0 (6.8 to 21.8) g (P for linear trend=0.002); however, mean haemoglobin was not associated with the risk of low birth weight and preterm birth. No evidence of a significant effect on duration of gestation, small for gestational age births, and birth length was noted.
Conclusions: Daily prenatal use of iron substantially improved birth weight in a linear dose-response fashion, probably leading to a reduction in risk of low birth weight. An improvement in prenatal mean haemoglobin concentration linearly increased birth weight.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at
Figures
Comment in
-
Iron supplementation in pregnancy.BMJ. 2013 Jul 10;347:f4399. doi: 10.1136/bmj.f4399. BMJ. 2013. PMID: 23843551 No abstract available.
References
-
- Stoltzfus R, Dreyfuss M. Guidelines for the use of iron supplements to prevent and treat iron deficiency anaemia. ILSI Press, 1998.
-
- World Health Organization. Micronutrient deficiencies: iron deficiency anaemia. www.who.int/nutrition/topics/ida/en/.
-
- World Health Organization. The prevalence of anaemia in women: a tabulation of available information (WHO/MCH/MSM/92). 2nd ed. WHO, Maternal Health and Safe Motherhood Programme, Division of Family Health, 1992.
-
- Institute of Medicine. Iron deficiency anemia: guidelines for prevention, detection and management among U.S. children and women of childbearing age. National Academy Press, 1993. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical