

Prognostication of recovery time after acute peripheral facial palsy: a prospective cohort study
- PMID: 23794548
- PMCID: PMC3669721
- DOI: 10.1136/bmjopen-2013-003007
Prognostication of recovery time after acute peripheral facial palsy: a prospective cohort study
Abstract
Objective: Owing to a lack of prospective studies, our aim was to evaluate diagnostic factors, in particular, motor and non-motor function tests, for prognostication of recovery time in patients with acute facial palsy (AFP).
Design: Prospective cohort study.
Setting: University hospital.
Participants: 259 patients with AFP.
Measurements: Clinical data, facial grading, electrophysiological motor function tests and other non-motor function tests were assessed for their contribution to recovery time.
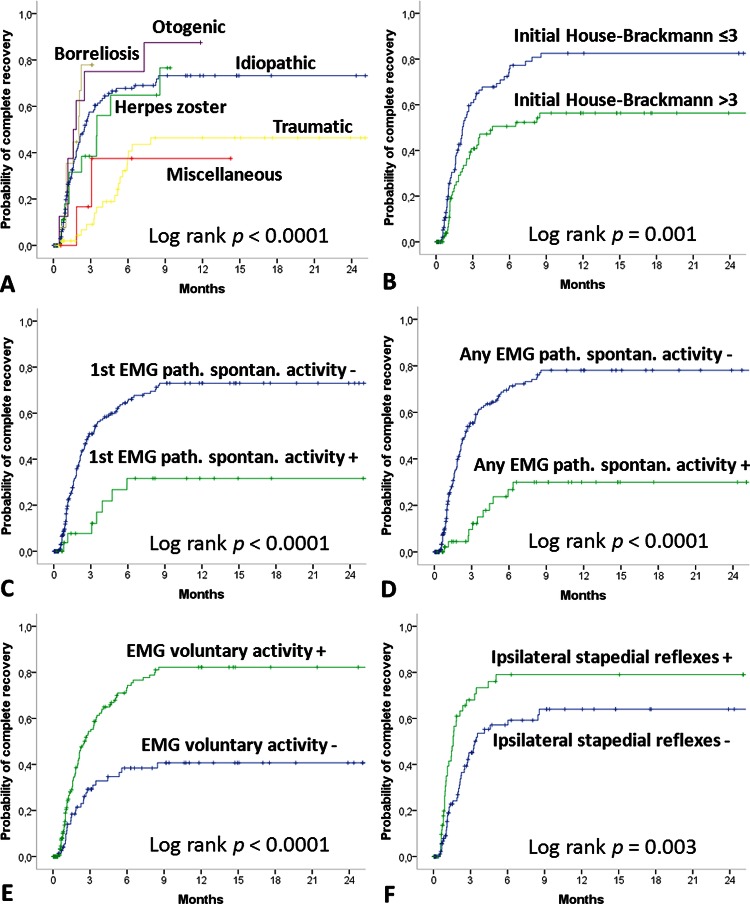
Results: The predominant origin of AFP was idiopathic (59%) and traumatic (21%). At baseline, the House-Brackmann scale (HB) was >III in 46% of patients. Follow-up time was 5.6±9.8 months with a complete recovery rate of 49%. The median recovery time was 3.5 months (95% CI 2.2 to 4.7 months). The following variables were associated with faster recovery: Interval between onset of AFP and treatment <6 days versus ≥6 days (median recovery time in months 2.1 vs 6.5; p<0.0001); HB ≤III vs >III (2.2 vs 4.6; p=0.001); no versus presence of pathological spontaneous activity in first electromyography (EMG; 2.8 vs probability of recovery <50%; p<0.0001); no versus voluntary activity in EMG (probability of recovery <50% vs 3.1; p<0.0001); normal versus pathological ipsilateral electroneurography (1.9 vs 6.5; p=0.008), normal versus pathological stapedius reflexes (1.6 vs 3.3; p=0.003).
Conclusions: Start of treatment and grading, but most importantly EMG evaluated for pathological spontaneous activity and the stapedius reflex test are powerful prognosticators for estimating the recovery time from AFP. These results need confirmation in larger datasets.
Keywords: Neurophysiology.
Figures
References
-
- Gilden DH. Clinical practice. Bell's Palsy. N Engl J Med 2004;351:1323–31 - PubMed
-
- Heckmann JG, Lang C, Glocker FX, et al. The new S2k AWMF guideline for the treatment of Bell's palsy in commented short form. Laryngorhinootologie 2012;91:686–92 - PubMed
-
- Sullivan FM, Swan IR, Donnan PT, et al. Early treatment with prednisolone or acyclovir in Bell's palsy. N Engl J Med 2007;357:1598–607 - PubMed
-
- Hato N, Yamada H, Kohno H, et al. Valacyclovir and prednisolone treatment for Bell's palsy: a multicenter, randomized, placebo-controlled study. Otol Neurotol 2007;28:408–13 - PubMed
-
- Engstrom M, Berg T, Stjernquist-Desatnik A, et al. Prednisolone and valaciclovir in Bell's palsy: a randomised, double-blind, placebo-controlled, multicentre trial. Lancet Neurol 2008;7:993–1000 - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources