

Pediatric flexible flatfoot; clinical aspects and algorithmic approach
- PMID: 23795246
- PMCID: PMC3684468
Pediatric flexible flatfoot; clinical aspects and algorithmic approach
Abstract
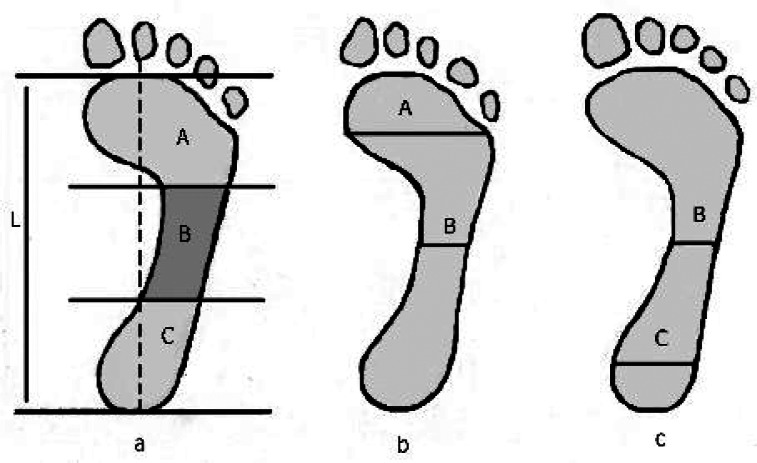
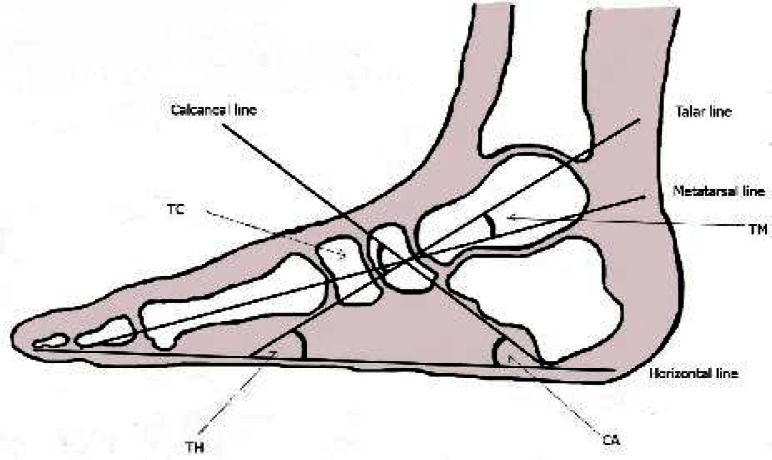
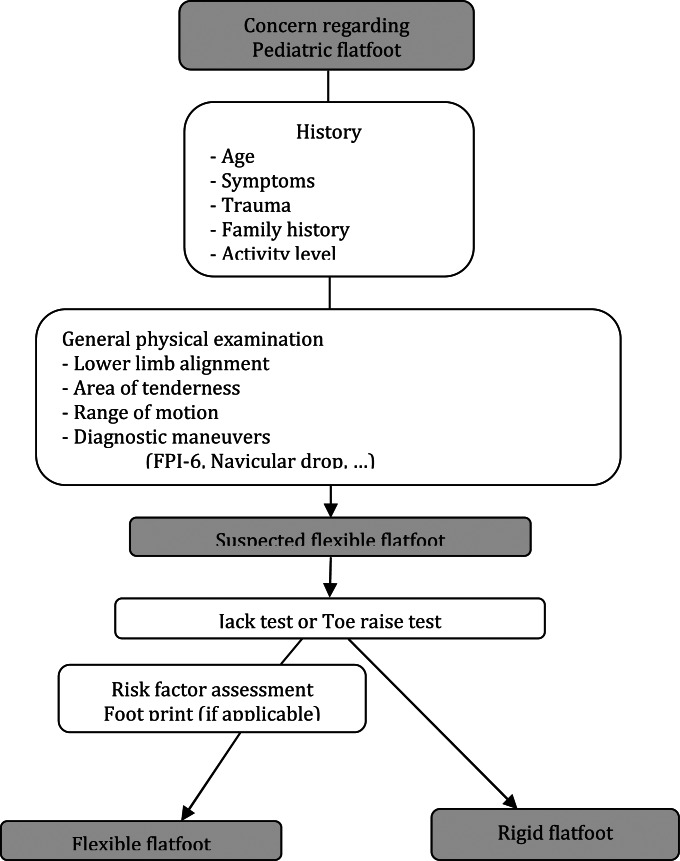
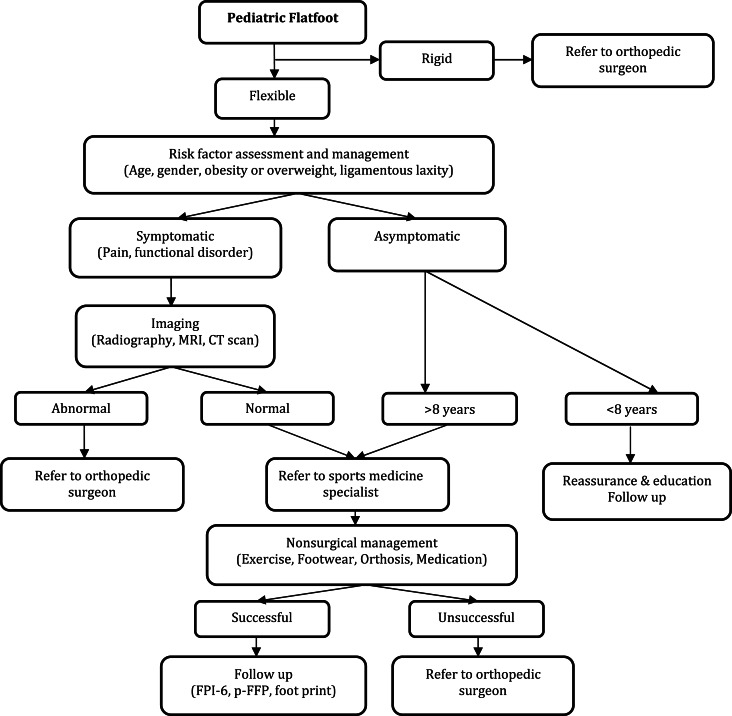
Flatfoot constitutes the major cause of clinic visits for pediatric foot problems. The reported prevalence of flatfoot varies widely due to numerous factors. It can be divided into flexible and rigid flatfoot. Diagnosis and management of pediatric flatfoot has long been the matter of controversy. Common assessment tools include visual inspection, anthropometric values, footprint parameters and radiographic evaluation. Most flexible flatfeet are physiologic, asymptomatic, and require no treatment. Otherwise, the physician should treat symptomatic flexible flatfeet. Initial treatment options include activity modification, proper shoe and orthoses, exercises and medication. Furthermore, comorbidities such as obesity and ligamenous laxity should be identified and managed, if applicable. When all nonsurgical treatment options faile, surgery can be considered. Our purpose in this article is to present a clinical algorithmic approach to pediatric flatfoot.
Keywords: Algorithm; Children; Exercise; Flatfoot; Hyperpronation; Orthosis; Pes planus.
Figures
References
-
- Fabry G. Clinical practice. Static, axial, and rotational deformities of the lower extremities in children. Eur J Pediatr. 2010;169(5):529–34. - PubMed
-
- Krul M, van der Wouden JC, Schellevis FG, et al. Foot problems in children presented to the family physician: a comparison between 1987 and 2001. Fam Pract. 2009;26(3):174–9. - PubMed
-
- Lin CJ, Lai KA, Kuan TS, et al. Correlating factors and clinical significance of flexible flatfoot in preschool children. J Pediatr Orthop. 2001;21(3):378–82. - PubMed
-
- Pfeiffer M, Kotz R, Ledl T, et al. Prevalence of flat foot in preschool-aged children. Pediatrics. 2006;118(2):634–9. - PubMed
LinkOut - more resources
Full Text Sources