

Systematic review of genuine versus spurious side-effects of beta-blockers in heart failure using placebo control: recommendations for patient information
- PMID: 23796325
- PMCID: PMC3819624
- DOI: 10.1016/j.ijcard.2013.05.068
Systematic review of genuine versus spurious side-effects of beta-blockers in heart failure using placebo control: recommendations for patient information
Abstract
Background: Patients trying life-preserving agents such as beta-blockers may be discouraged by listings of harmful effects provided in good faith by doctors, drug information sheets, and media. We systematically review the world experience of side-effect information in blinded, placebo-controlled beta-blockade in heart failure. We present information for a physician advising a patient experiencing an unwanted symptom and suspecting the drug.
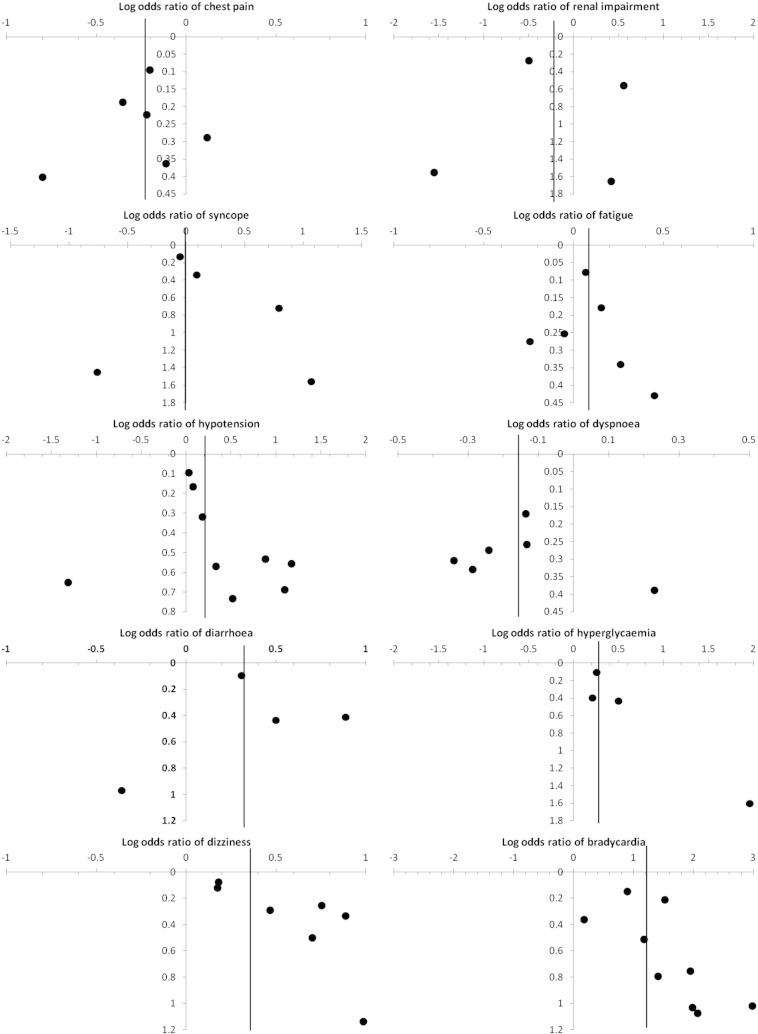
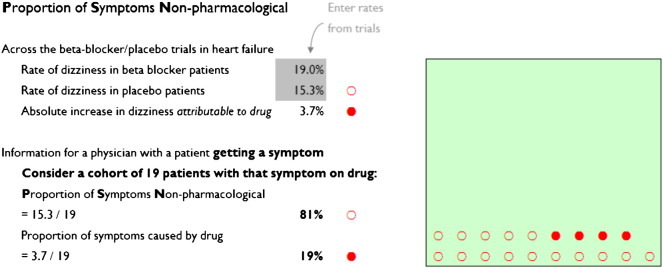
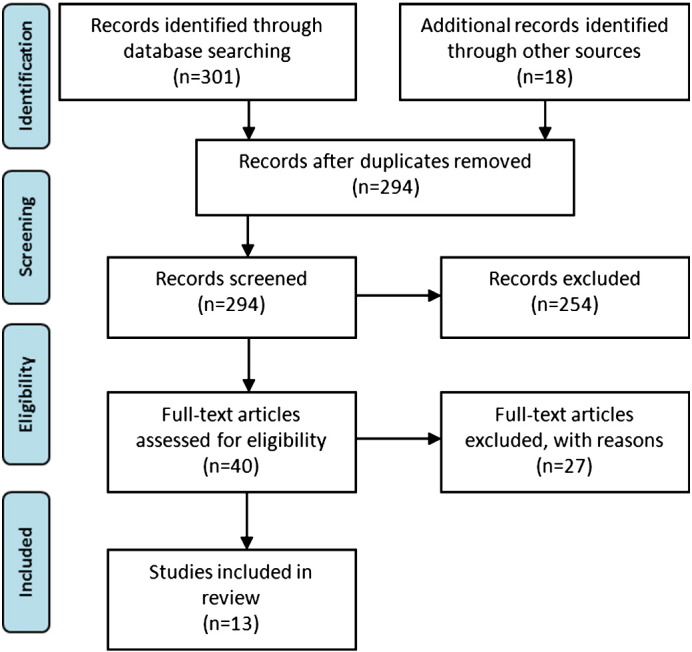
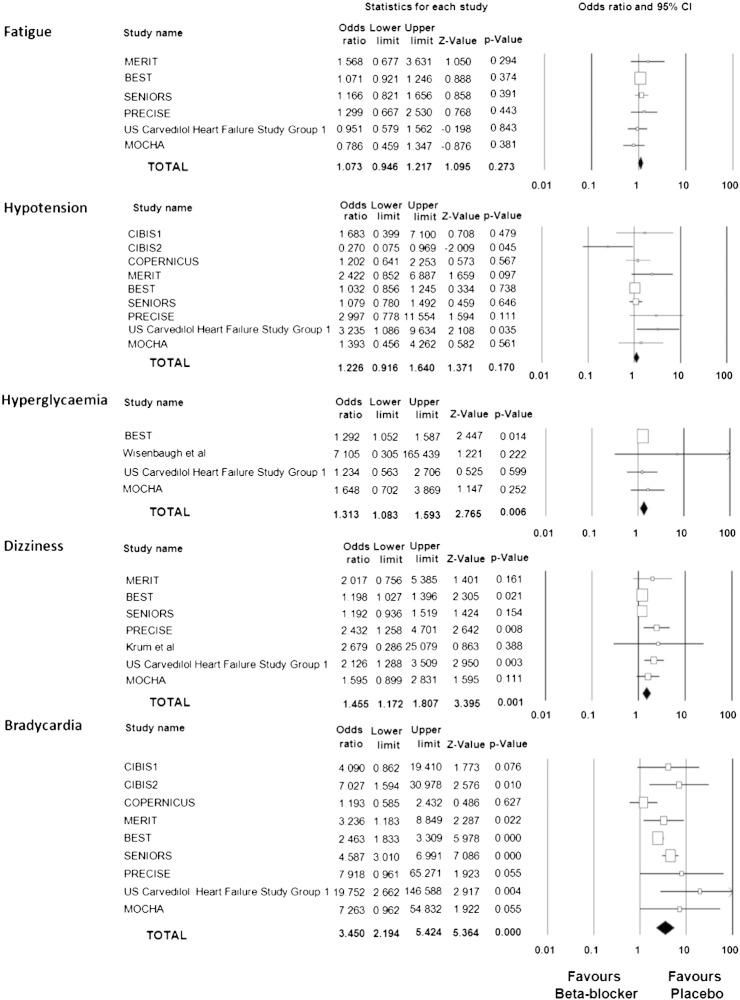
Methods: We searched Medline for double-blinded randomized trials of beta-blocker versus placebo in heart failure reporting side-effects. We calculated, per 100 patients reporting the symptom on beta-blockade, how many would have experienced it on placebo: the "proportion of symptoms non-pharmacological".
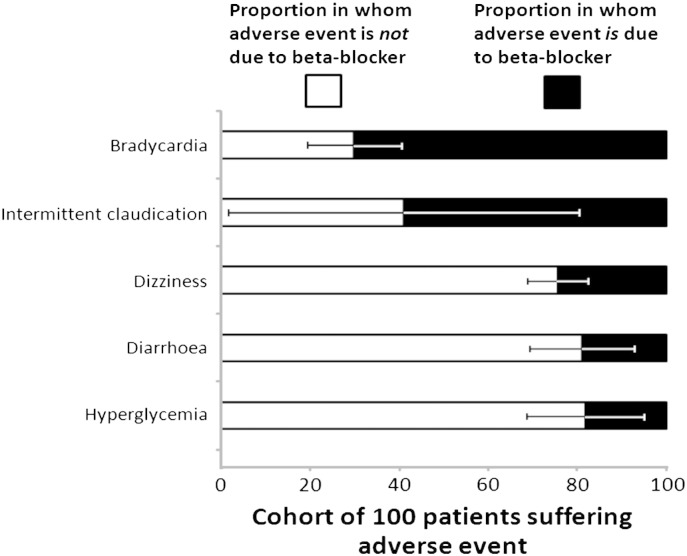
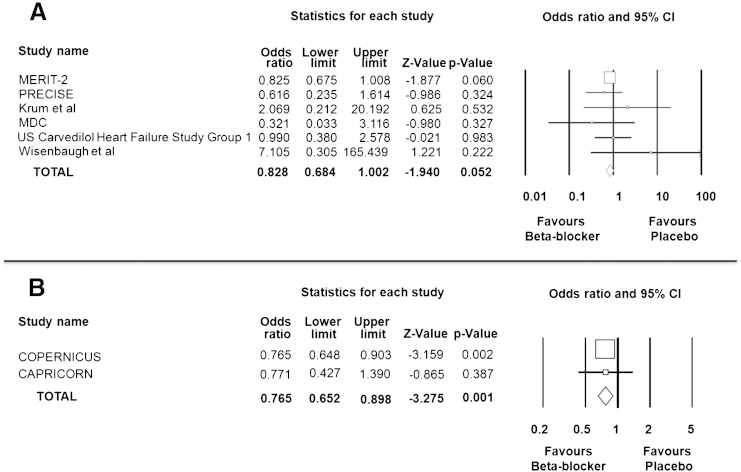
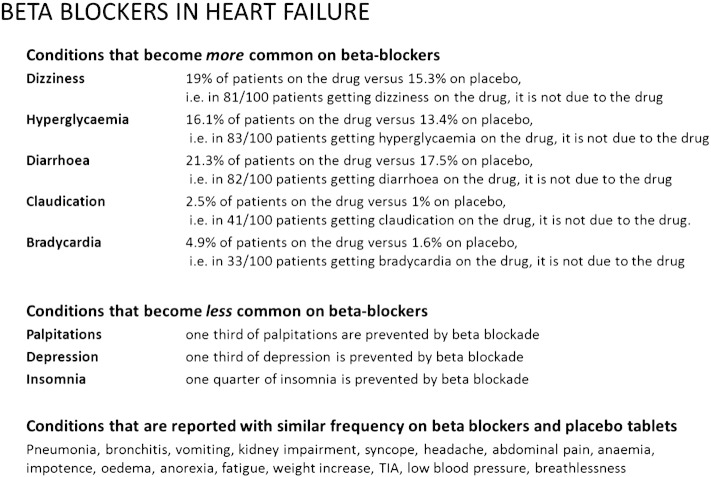
Results: 28 of the 33 classically-described side-effects are not significantly more common on beta-blockers than placebo. Of the 100 patients developing dizziness on beta-blockers, 81 (95% CI 73-89) would have developed it on placebo. For diarrhoea this proportion is 82/100 (70-95), and hyperglycaemia 83/100 (68-98). For only two side-effects is this under half (i.e. predominantly due to beta-blocker): bradycardia (33/100, CI 21-44) and intermittent claudication (41/100, 2-81). At least 6 so-called side-effects are less common on beta-blocker than placebo, including depression (reduced by 35%, p<0.01) and insomnia (by 27%, p=0.01).
Conclusions: Clinicians might reconsider whether it is scientifically and ethically correct to warn a patient that a drug might cause them a certain side-effect, when randomized controlled trials show no significant increase, or indeed a significant reduction. A better informed consultation could, in patients taking beta-blockers, alleviate suffering. In patients who might otherwise not take the drug, it might prevent deaths.
Keywords: Beta-blockers; Heart failure; Side-effects.
Copyright © 2013 The Authors. Published by Elsevier Ireland Ltd.. All rights reserved.
Figures
References
-
- CIBIS II Study Group The cardiac insufficiency bisoprolol study II (CIBIS II): a randomized trial. Lancet. 1999;353:9–13. - PubMed
-
- Packer M., Fowler M.B., Roecker E.B. Effect of carvedilol on the morbidity of patients with severe chronic heart failure: results of the carvedilol prospective randomized cumulative survival (COPERNICUS) study. Circulation. 2002;106(17):2194–2199. - PubMed
-
- Cleland J.G., McDonagh T., Rigby A.S., Yassin A., Whittaker T., Dargie H.J. National Heart Failure Audit Team for England and Wales. The national heart failure audit for England and Wales 2008–2009. Heart. Jun 2011;97(11):876–886. - PubMed
-
- http://www.medicines.org.uk/emc. 2011 Datapharm Communications Ltd.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
