

Clinical Outcomes in Patients with Heterogeneous Vancomycin-Intermediate Staphylococcus aureus Bloodstream Infection
- PMID: 23796929
- PMCID: PMC3754327
- DOI: 10.1128/AAC.00380-13
Clinical Outcomes in Patients with Heterogeneous Vancomycin-Intermediate Staphylococcus aureus Bloodstream Infection
Abstract
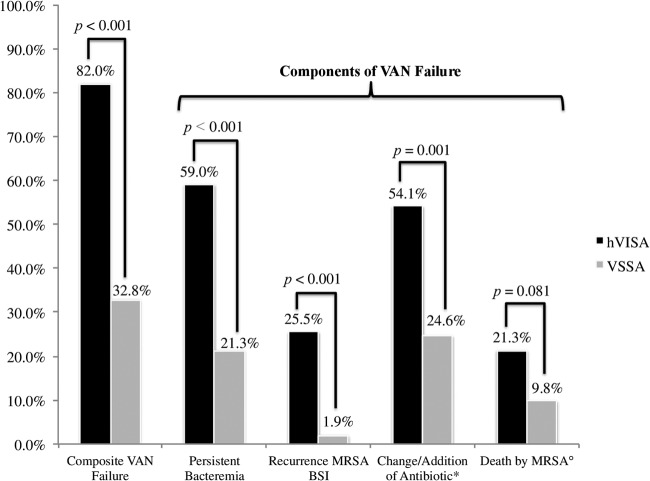
The prevalence of heterogeneous vancomycin-intermediate Staphylococcus aureus (hVISA) infections varies in the literature, a problem complicated by the lack of routine screening procedures; however, limited data suggest that hVISA has been associated with persistent bloodstream infections (BSI) and vancomycin failure, yet these studies have been confounded by design issues. We conducted this study to compare the characteristics of patients with BSI caused by hVISA with those with vancomycin-susceptible Staphylococcus aureus (VSSA) treated with vancomycin. This retrospective, multicenter matched (1:1) cohort study compared the clinical characteristics and outcomes of hVISA and VSSA. Patients with hVISA methicillin-resistant Staphylococcus aureus (MRSA) BSI from 2004 to 2012 were matched to VSSA-MRSA BSI patients. The primary outcome was failure of vancomycin treatment, defined as a composite of persistent bacteremia (≥7 days), persistent signs and symptoms, change of MRSA antibiotic, recurrent BSI, or MRSA-related mortality. We identified 122 matched cases. The overall vancomycin failure rate was 57% (82% hVISA versus 33% VSSA; P < 0.001). The individual components of failure in hVISA versus VSSA were persistent bacteremia, 59% versus 21% (P < 0.001); change in MRSA therapy, 54% versus 25% (P = 0.001); MRSA-related mortality, 21% versus 10% (P = 0.081); and recurrence of BSI, 26% versus 2% (P < 0.001). Using logistic regression analysis and adjusting for covariates, hVISA (adjusted odds ratio [aOR], 11.1; 95% confidence interval [CI], 4.3 to 28.7) and intensive care unit (ICU) admission (aOR, 4.5; 95% CI, 1.8 to 11.6) were still independently associated with vancomycin failure. Relative to VSSA BSI, patients with hVISA were more likely to experience failure of vancomycin treatment, including persistent bacteremia and recurrence. Our results indicate that hVISA was responsible for considerable morbidity.
Copyright © 2013, American Society for Microbiology. All Rights Reserved.
Figures
References
-
- Sakoulas G, Gold HS, Cohen RA, Venkataraman L, Moellering RC, Eliopoulos GM. 2006. Effects of prolonged vancomycin administration on methicillin-resistant Staphylococcus aureus (MRSA) in a patient with recurrent bacteraemia. J. Antimicrob. Chemother. 57:699–704 - PubMed
-
- Liu C, Bayer A, Cosgrove SE, Daum RS, Fridkin SK, Gorwitz RJ, Kaplan SL, Karchmer AW, Levine DP, Murray BEJRM, Talan DA, Chambers HF. 2011. Clinical practice guidelines by the Infectious Diseases Society of America for the treatment of methicillin-resistant Staphylococcus aureus infections in adults and children. Clin. Infect. Dis. 52:e18–e55 - PubMed
-
- Hiramatsu K, Hanaki H, Ino T, Yabuta K, Oguri T, Tenover FC. 1997. Methicillin-resistant Staphylococcus aureus clinical strain with reduced vancomycin susceptibility. J. Antimicrob. Chemother. 40:135–136 - PubMed
-
- Centers for Disease Control and Prevention 2002. Staphylococcus aureus resistant to vancomycin—United States, 2002. MMWR Morb. Mortal. Wkly. Rep. 51:565–567 - PubMed
-
- Fridkin SK, Hageman J, McDougal LK, Mohammed J, Jarvis WR, Perl TM, Tenover FC. 2003. Epidemiological and microbiological characterization of infections caused by Staphylococcus aureus with reduced susceptibility to vancomycin, United States, 1997-2001. Clin. Infect. Dis. 36:429–439 - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
