

Right ventricular dysfunction in systemic sclerosis-associated pulmonary arterial hypertension
- PMID: 23797369
- PMCID: PMC3815697
- DOI: 10.1161/CIRCHEARTFAILURE.112.000008
Right ventricular dysfunction in systemic sclerosis-associated pulmonary arterial hypertension
Abstract
Background: Systemic sclerosis–associated pulmonary artery hypertension (SScPAH) has a worse prognosis compared with idiopathic pulmonary arterial hypertension (IPAH), with a median survival of 3 years after diagnosis often caused by right ventricular (RV) failure. We tested whether SScPAH or systemic sclerosis–related pulmonary hypertension with interstitial lung disease imposes a greater pulmonary vascular load than IPAH and leads to worse RV contractile function.
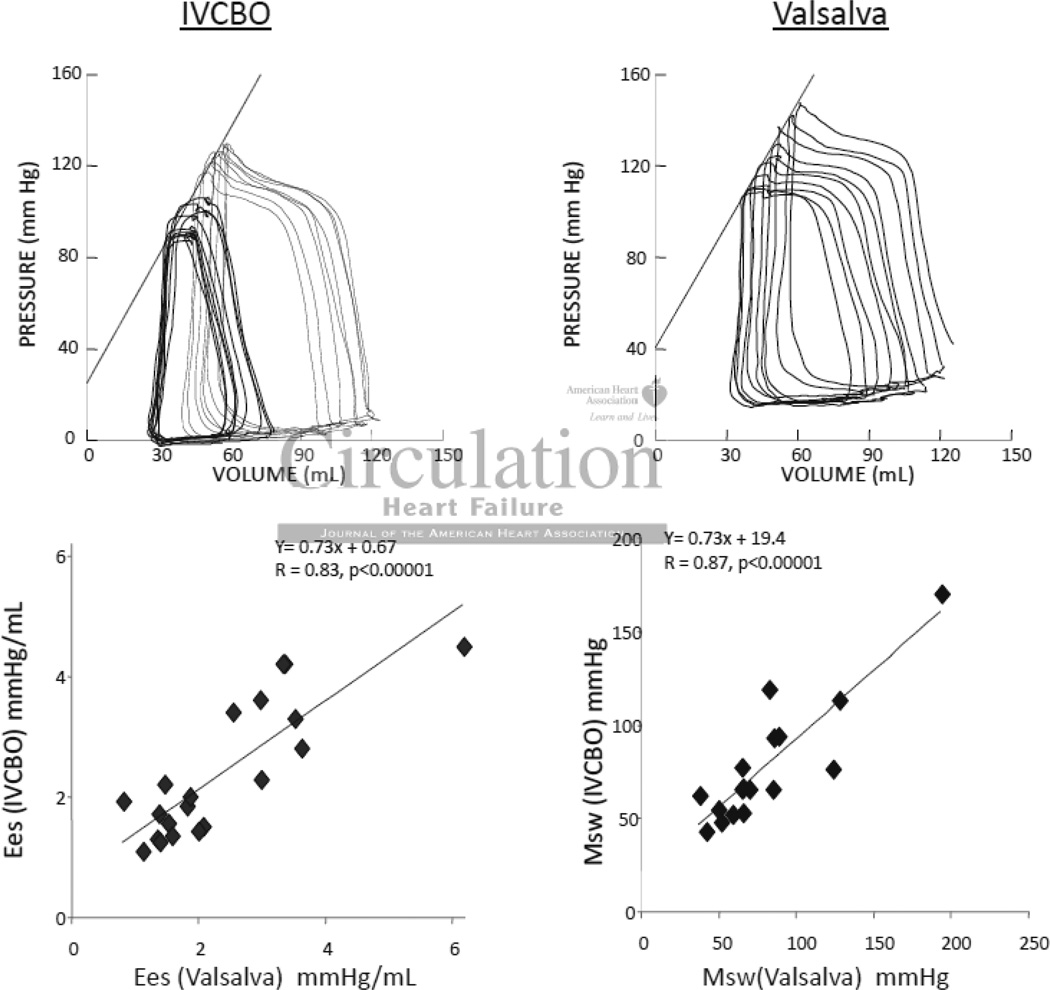
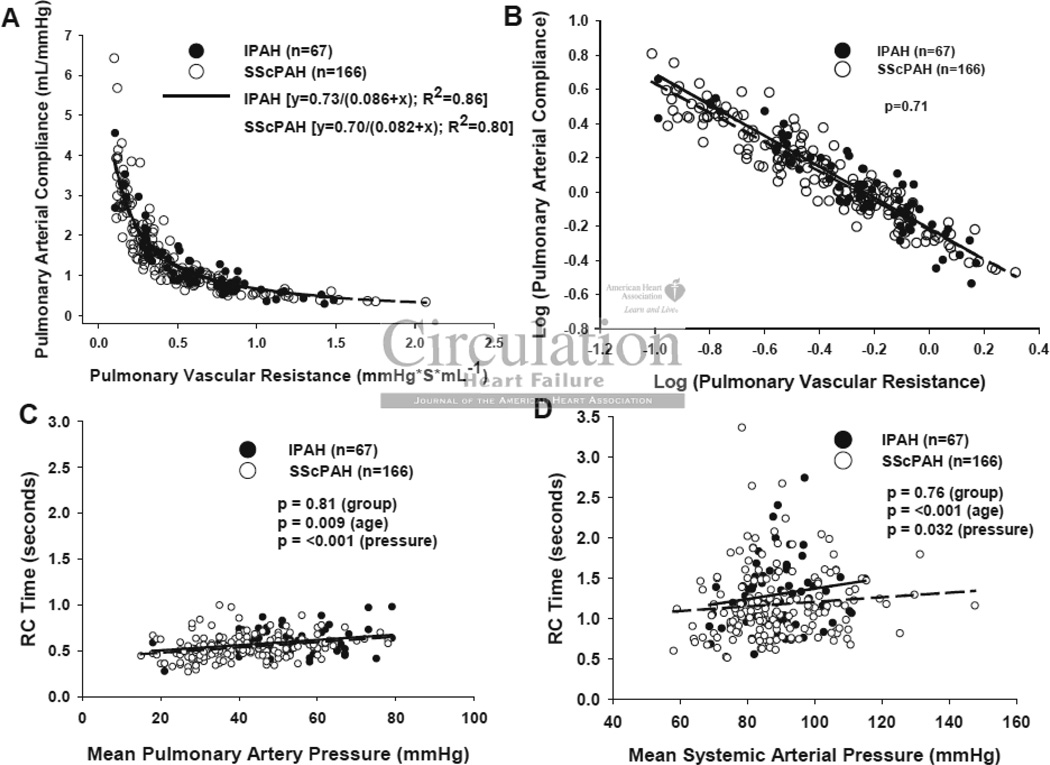
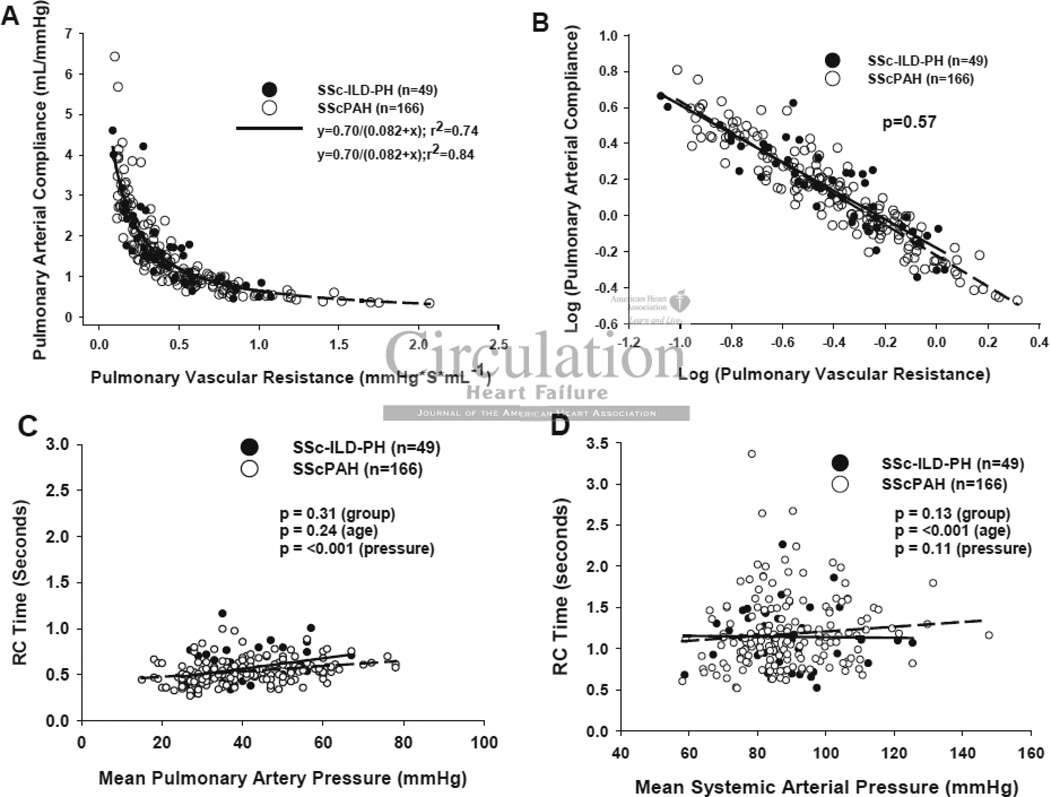
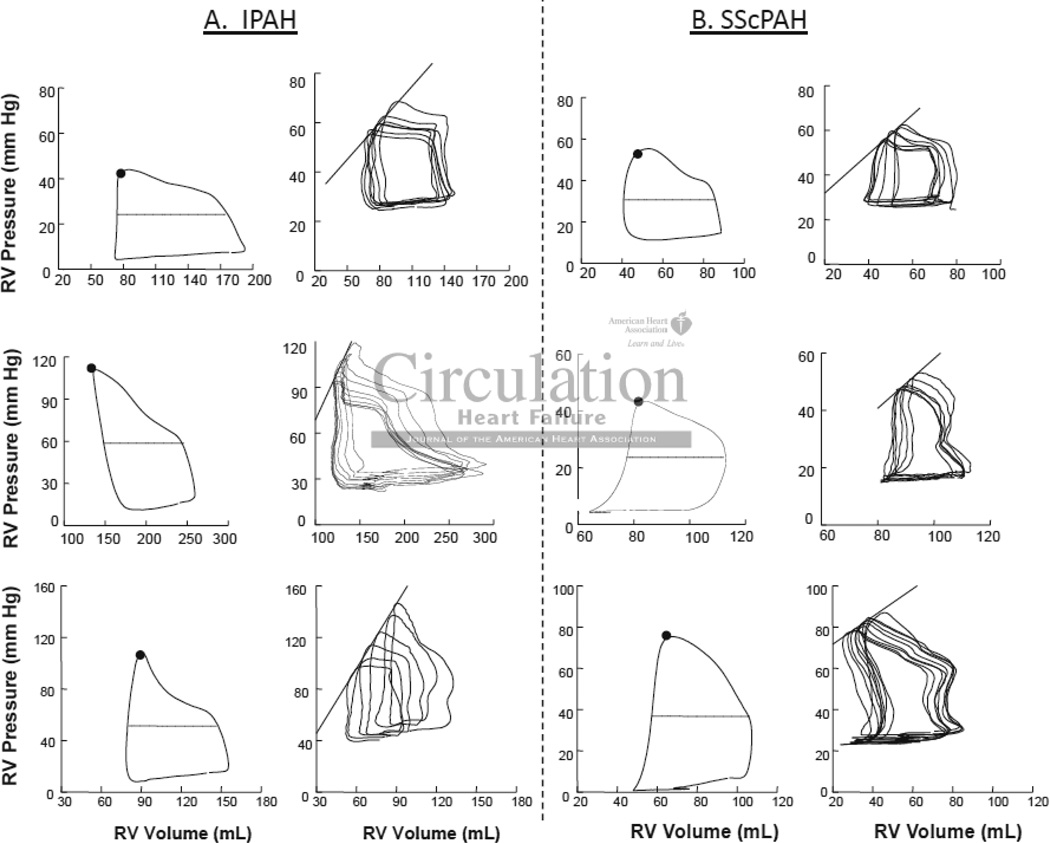
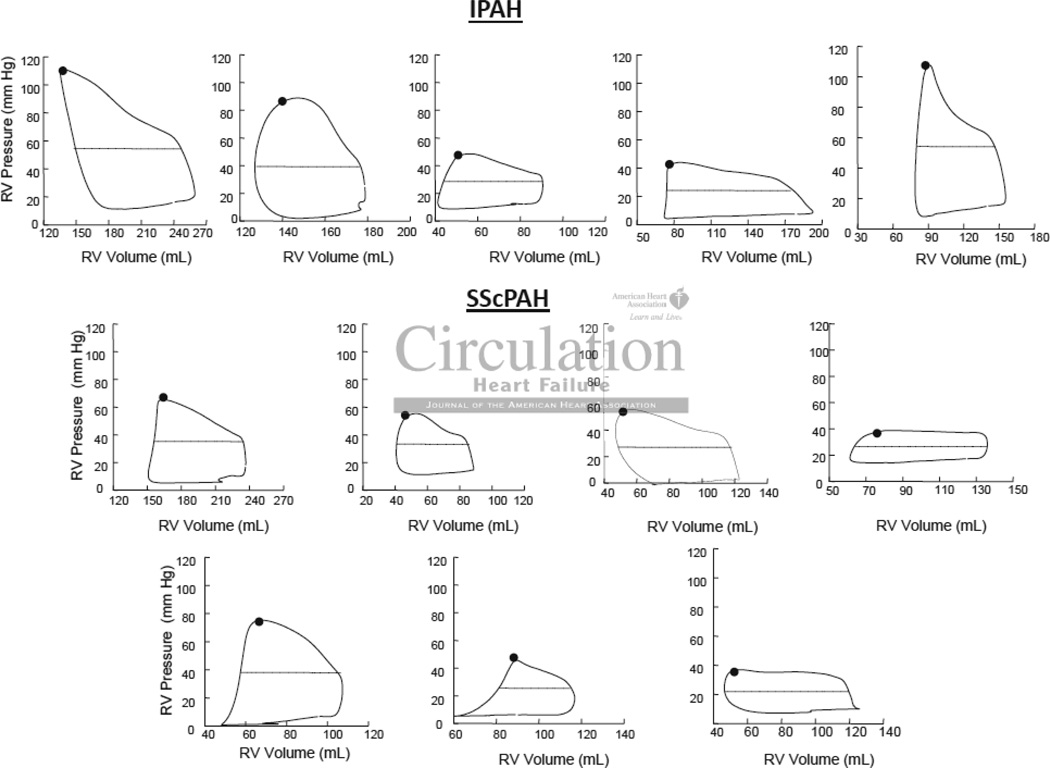
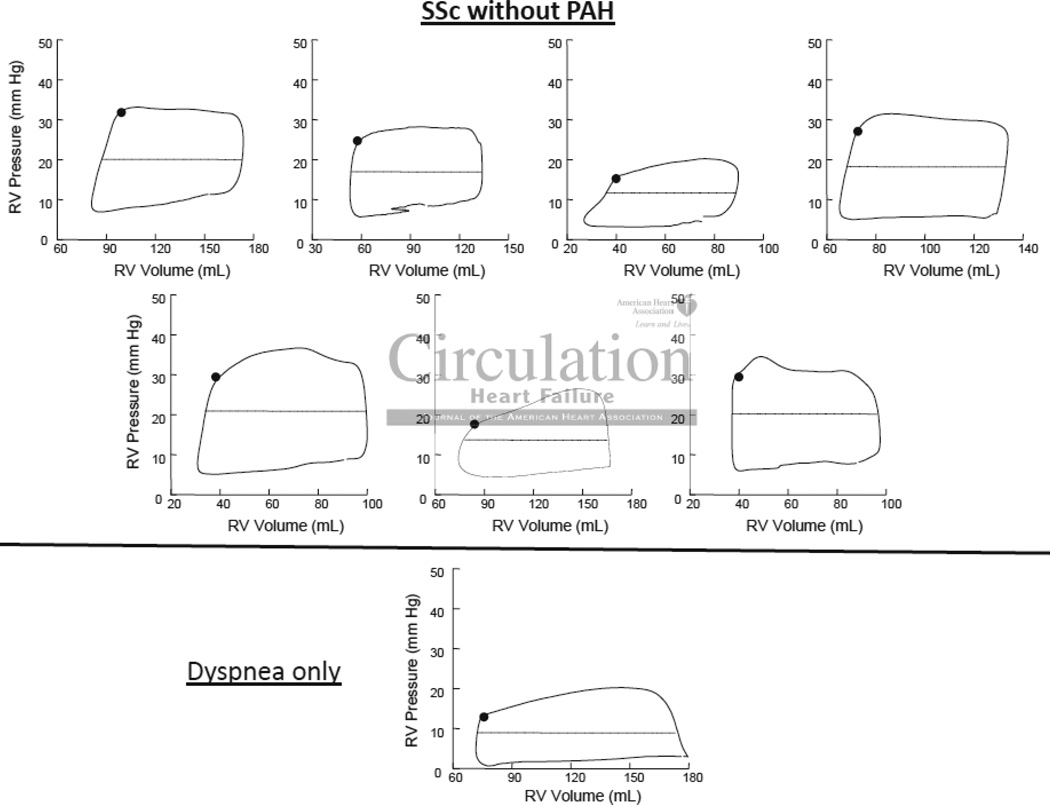
Methods and results: We analyzed pulmonary artery pressures and mean flow in 282 patients with pulmonary hypertension (166 SScPAH, 49 systemic sclerosis–related pulmonary hypertension with interstitial lung disease, and 67 IPAH). An inverse relation between pulmonary resistance and compliance was similar for all 3 groups, with a near constant resistance×compliance product. RV pressure–volume loops were measured in a subset, IPAH (n=5) and SScPAH (n=7), as well as SSc without PH (n=7) to derive contractile indexes (end-systolic elastance [Ees] and preload recruitable stroke work [Msw]), measures of RV load (arterial elastance [Ea]), and RV pulmonary artery coupling (Ees/Ea). RV afterload was similar in SScPAH and IPAH (pulmonary vascular resistance=7.0±4.5 versus 7.9±4.3 Wood units; Ea=0.9±0.4 versus 1.2±0.5 mm Hg/mL; pulmonary arterial compliance=2.4±1.5 versus 1.7±1.1 mL/mm Hg; P>0.3 for each). Although SScPAH did not have greater vascular stiffening compared with IPAH, RV contractility was more depressed (Ees=0.8±0.3 versus 2.3±1.1, P<0.01; Msw=21±11 versus 45±16, P=0.01), with differential RV-PA uncoupling (Ees/Ea=1.0±0.5 versus 2.1±1.0; P=0.03). This ratio was higher in SSc without PH (Ees/Ea=2.3±1.2; P=0.02 versus SScPAH).
Conclusions: RV dysfunction is worse in SScPAH compared with IPAH at similar afterload, and may be because of intrinsic systolic function rather than enhanced pulmonary vascular resistive and pulsatile loading.
Figures
References
-
- Overbeek MJ, Vonk MC, Boonstra A, Voskuyl AE, Vonk-Noordegraaf A, Smit EF, Dijkmans BAC, Postmus PE, Mooi WJ, Heijdra Y, Grünberg K. Pulmonary arterial hypertension in limited cutaneous systemic sclerosis: a distinctive vasculopathy. European Respiratory Journal. 2009;34:371–379. - PubMed
-
- Haddad F, Doyle R, Murphy DJ, Hunt SA. Right Ventricular Function in Cardiovascular Disease, Part II. Circulation. 2008;117:1717–1731. - PubMed
-
- Hesselstrand R, Wildt M, Ekmehag B, Wuttge DM, Scheja A. Survival in patients with pulmonary arterial hypertension associated with systemic sclerosis from a Swedish single centre: prognosis still poor and prediction difficult. Scand J Rheumatol. 2011;40:127–132. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
