

Treatment outcomes in AIDS-related diffuse large B-cell lymphoma in the setting roll out of combination antiretroviral therapy in South Africa
- PMID: 23797692
- PMCID: PMC3797444
- DOI: 10.1097/QAI.0b013e3182a03e9b
Treatment outcomes in AIDS-related diffuse large B-cell lymphoma in the setting roll out of combination antiretroviral therapy in South Africa
Abstract
Background: Long-term survival for patients with AIDS-related diffuse large B-cell lymphoma (DLBCL) is feasible in settings with available combination antiretroviral therapy (cART). However, given limited oncology resources, outcomes for AIDS-associated DLBCL in South Africa are unknown.
Methods: We performed a retrospective analysis of survival in patients with newly diagnosed AIDS-related DLBCL treated at a tertiary teaching hospital in Cape Town, South Africa, with cyclophosphamide, doxorubicin, vincristine, and oral prednisone (CHOP) or CHOP-like chemotherapy (January 2004 until December 2010). HIV-related and lymphoma-related prognostic factors were evaluated.
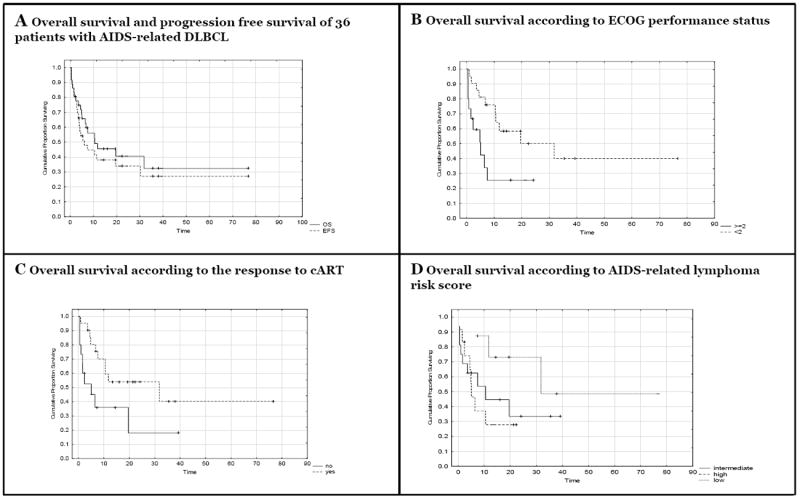
Results: Thirty-six patients evaluated; median age 37.3 years, 52.8% men, and 61.1% black South Africans. Median CD4 count 184 cells per microliter (in 27.8% this was <100 cells/μL), 80% high risk according to the age-adjusted International Prognostic Index. Concurrent Mycobacterium tuberculosis in 25%. Two-year overall survival (OS) was 40.5% (median OS 10.5 months, 95% confidence interval: 6.5 to 31.8). Eastern Cooperative Oncology Group performance status of 2 or more (25.4% vs 50.0%, P = 0.01) and poor response to cART (18.0% vs 53.9%, P = 0.03) predicted inferior 2-year OS. No difference in 2-year OS was demonstrated in patients coinfected with M. tuberculosis (P = 0.87).
Conclusions: Two-year OS for patients with AIDS-related DLBCL treated with CHOP like regimens and cART is comparable to that seen in the United States and Europe. Important factors effecting OS in AIDS-related DLBCL in South Africa include performance status at presentation and response to cART. Patients with comorbid M. tuberculosis or hepatitis B seropositivity seem to tolerate CHOP in our setting. Additional improvements in outcomes are likely possible.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures
References
-
- Gucalp A, Noy A. Spectrum of HIV lymphoma 2009. Curr Opin Hematol. 2010;17(4):362–367. - PubMed
-
- Sparano JA. HIV-associated lymphoma: The evidence for treating aggressively but with caution. Curr Opin Oncol. 2007;19(5):458–463. - PubMed
-
- Mantina H, Wiggill TM, Carmona S, Perner Y, Stevens WS. Characterization of lymphomas in a high prevalence HIV setting. J Acquir Immune Defic Syndr. 2010;53(5):656–660. - PubMed
-
- Abayomi EA, Somers A, Grewal R, et al. Impact of the HIV epidemic and anti-retroviral treatment policy on lymphoma incidence and subtypes seen in the western cape of south africa, 2002-2009: Preliminary findings of the tygerberg lymphoma study group. Transfus Apher Sci. 2011;44(2):161–166. - PMC - PubMed
-
- Gottlieb JA, Gutterman JU, McCredie KB, Rodriguez V, Frei E., 3rd Chemotherapy of malignant lymphoma with adriamycin. Cancer Res. 1973;33(11):3024–3028. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
