

Much of late life cognitive decline is not due to common neurodegenerative pathologies
- PMID: 23798485
- PMCID: PMC3845973
- DOI: 10.1002/ana.23964
Much of late life cognitive decline is not due to common neurodegenerative pathologies
Abstract
Objective: The pathologic indices of Alzheimer disease, cerebrovascular disease, and Lewy body disease accumulate in the brains of older persons with and without dementia, but the extent to which they account for late life cognitive decline remains unknown. We tested the hypothesis that these pathologic indices account for the majority of late life cognitive decline.
Methods: A total of 856 deceased participants from 2 longitudinal clinical-pathologic studies, Rush Memory and Aging Project and Religious Orders Study, completed a mean of 7.5 annual evaluations, including 17 cognitive tests. Neuropathologic examinations provided quantitative measures of global Alzheimer pathology, amyloid load, tangle density, macroscopic infarcts, microinfarcts, and neocortical Lewy bodies. Random coefficient models were used to examine the linear relation of pathologic indices with global cognitive decline. In subsequent analyses, random change point models were used to examine the relation of the pathologic indices with the onset of terminal decline and rates of preterminal and terminal decline (ie, nonlinear decline).
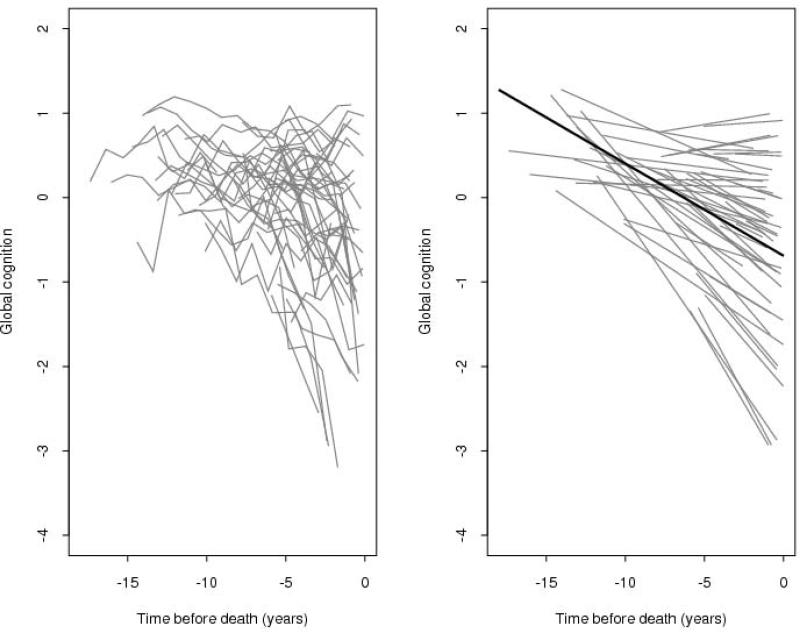
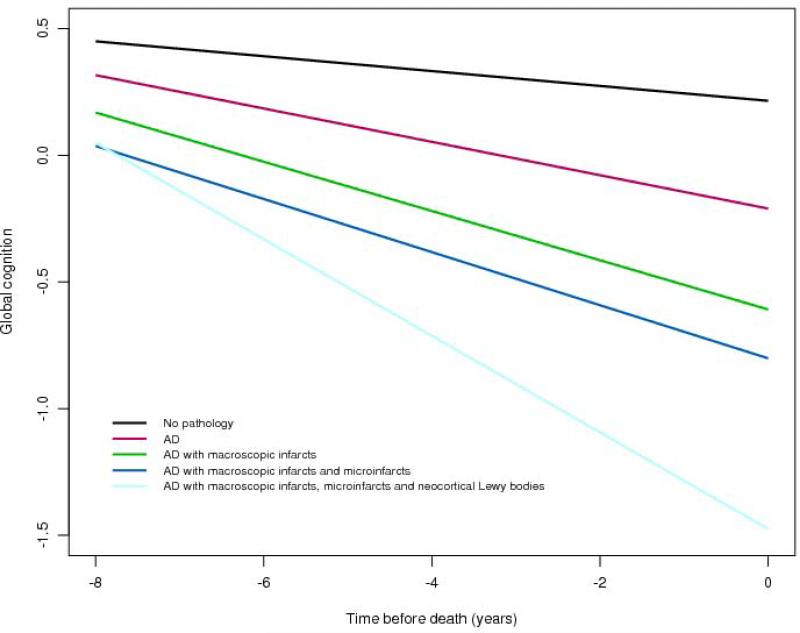
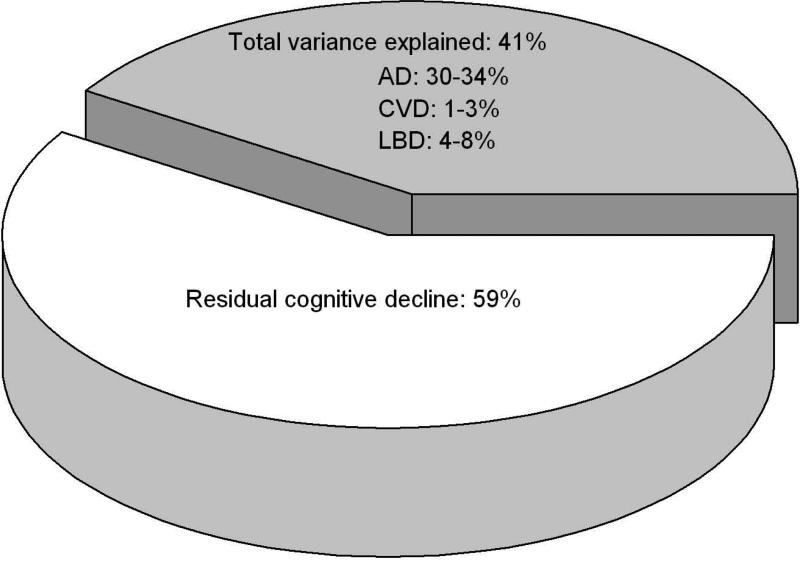
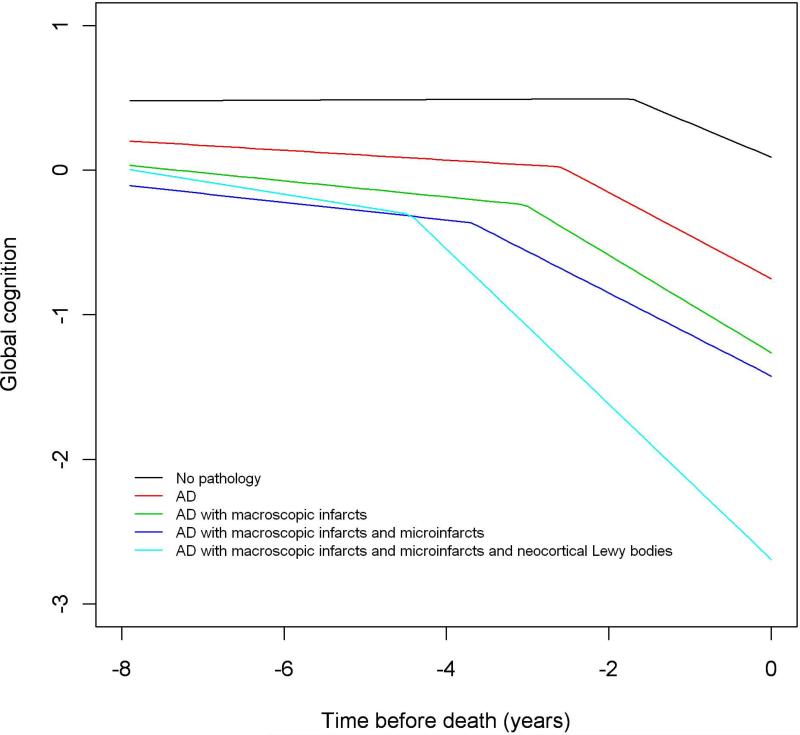
Results: Cognition declined a mean of about 0.11 U per year (estimate = -0.109, standard error [SE] = 0.004, p < 0.001), with significant individual differences in rates of decline; the variance estimate for the individual slopes was 0.013 (SE = 0.112, p < 0.001). In separate analyses, global Alzheimer pathology, amyloid, tangles, macroscopic infarcts, and neocortical Lewy bodies were associated with faster rates of decline and explained 22%, 6%, 34%, 2%, and 8% of the variation in decline, respectively. When analyzed simultaneously, the pathologic indices accounted for a total of 41% of the variation in decline, and the majority remained unexplained. Furthermore, in random change point models examining the influence of the pathologic indices on the onset of terminal decline and the preterminal and terminal components of the cognitive trajectory, the common pathologic indices accounted for less than a third of the variation in the onset of terminal decline and rates of preterminal and terminal decline.
Interpretation: The pathologic indices of the common causes of dementia are important determinants of cognitive decline in old age and account for a large proportion of the variation in late life cognitive decline. Surprisingly, however, much of the variation in cognitive decline remains unexplained, suggesting that other important determinants of cognitive decline remain to be identified. Identification of the mechanisms that contribute to the large unexplained proportion of cognitive decline is urgently needed to prevent late life cognitive decline.
Copyright © 2013 American Neurological Association.
Figures
Comment in
-
Age, rate of change in neuropathology, and trajectory of cognitive decline.Ann Neurol. 2014 Mar;75(3):455-6. doi: 10.1002/ana.24038. Epub 2014 Mar 4. Ann Neurol. 2014. PMID: 24123067 No abstract available.
-
Reply: To PMID 23798485.Ann Neurol. 2014 Mar;75(3):456. doi: 10.1002/ana.24035. Epub 2014 Mar 4. Ann Neurol. 2014. PMID: 24596054 No abstract available.
References
-
- Wilson RS, Beckett LA, Barnes LL, et al. Individual differences in rates of change in cognitive abilities of older persons. Psych Aging. 2002;17:179–193. - PubMed
-
- Wilson RS, Li Y, Bienias JL, Bennett DA. Cognitive decline in old age: Separating practice effects from the effects of growing older. Psych Aging. 2006;21:774–789. - PubMed
-
- Sonnen JA, Larson EB, Crane PK, et al. Pathological correlates of dementia in a longitudinal, population-based sample of aging. Ann Neurol. 2007;62(4):406–13. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
