Keloid: A case report and review of pathophysiology and differences between keloid and hypertrophic scars
- PMID: 23798844
- PMCID: PMC3687166
- DOI: 10.4103/0973-029X.110701
Keloid: A case report and review of pathophysiology and differences between keloid and hypertrophic scars
Abstract
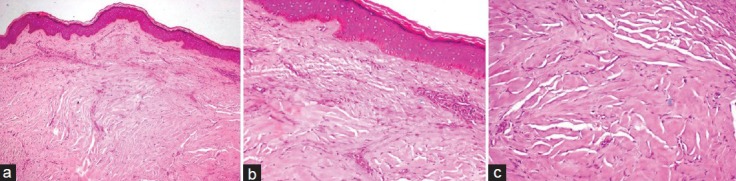
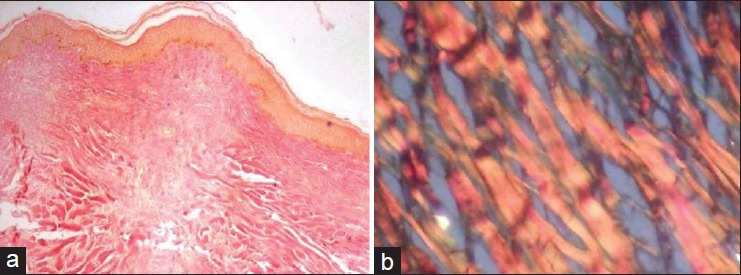
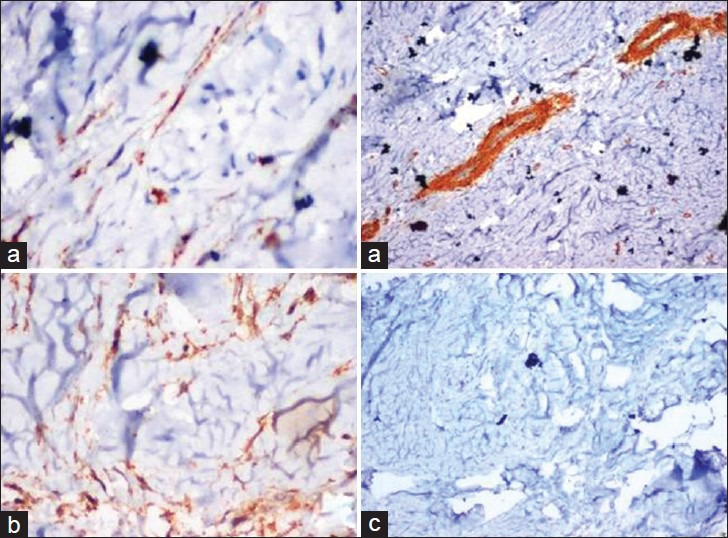
Keloids extend beyond the borders of the original wound invading normal skin. Usually appear as firm nodules, often pruritic and painful, and generally do not regress spontaneously. Most often occur on the chest, shoulders, upper back, back of the neck, and earlobes. The aim of the paper is to discuss a case of keloid, review the pathophysiology and also to highlight the differences between keloid and hypertrophic scars. A 26-year-old female complains of swelling on ear lobe since 3 years. Swelling was firm, non-tender, dumbell-shaped with central wooden stick still present, measuring 3 cm in diameter medial to the inferior part of the helix. A clinical diagnosis of keloid was given. Histopathological sections showed hyperorthokeratinized stratified squamous epithelium with deep dermal sclerosis showing large dense bundle of glassy collagen diagnostic of Keloid. Special stain like Van Gieson's was used to identify collagen bundles. The sections were also subjected to immunohistochemical markers such as α-SMA (alpha Smooth muscle actin), Desmin, and S-100. Despite decades of research, the pathophysiology of keloids remains incompletely understood. Recent studies indicate that TGF-β (Transforming growth factor beta) and PDGF (Platelet-derived growth factor) play an integral role in the formation of keloids. In future, development of selective inhibitors of TGF-β might produce new therapeutic tools with enhanced efficacy and specificity for the treatment of keloids. Patients with a previous history of keloid or other risk-factors should avoid body piercing and elective cosmetic procedures. Keloid scars should be sent for histopathology in order to avoid missing potentially malignant conditions particularly those showing unusual features.
Keywords: Ear lobe; fibrogenic response; glassy collagen; hypertrophic scars; keloid.
Conflict of interest statement
Figures

References
-
- Robles DT, Berg D. Abnormal wound healing: Keloids. Clin Dermatol. 2007;25:26–32. - PubMed
-
- Moshref SS, Mufti ST. Keloid and hypertrophic scars: Comparative histopathological and immunohistochemical study. Med Sci. 2010;17:3–22.
-
- Theopold C, Pritchard S, McGrouther DA, Bayat A. Keloid scar harbouring malignant blue naevus emphasises the need for excision biopsy and routine histology. J Plast Reconstr Aesthet Surg. 2009;62:93–5. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources