

Patterns of non-administration of ordered doses of venous thromboembolism prophylaxis: implications for novel intervention strategies
- PMID: 23799091
- PMCID: PMC3683023
- DOI: 10.1371/journal.pone.0066311
Patterns of non-administration of ordered doses of venous thromboembolism prophylaxis: implications for novel intervention strategies
Abstract
Background: Recent studies have documented high rates of non-administration of ordered venous thromboembolism (VTE) prophylaxis doses. Intervention strategies that target all patients have been effective, but prohibitively resource-intensive. We aimed to identify efficient intervention strategies based on patterns of non-administration of ordered VTE prophylaxis.
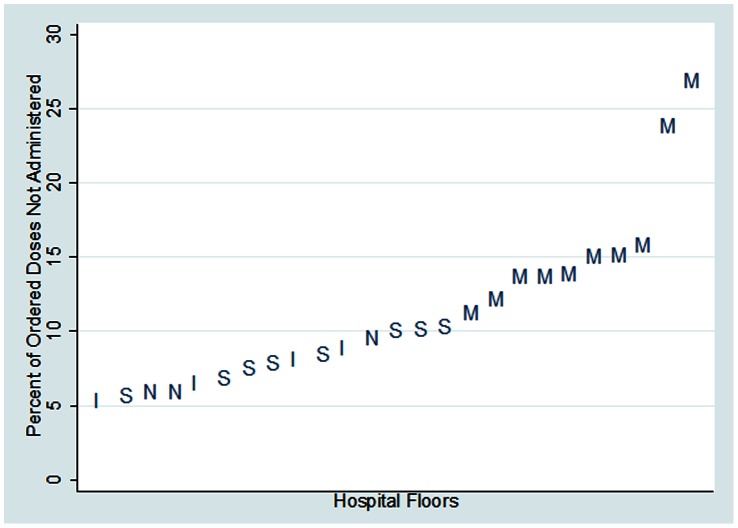
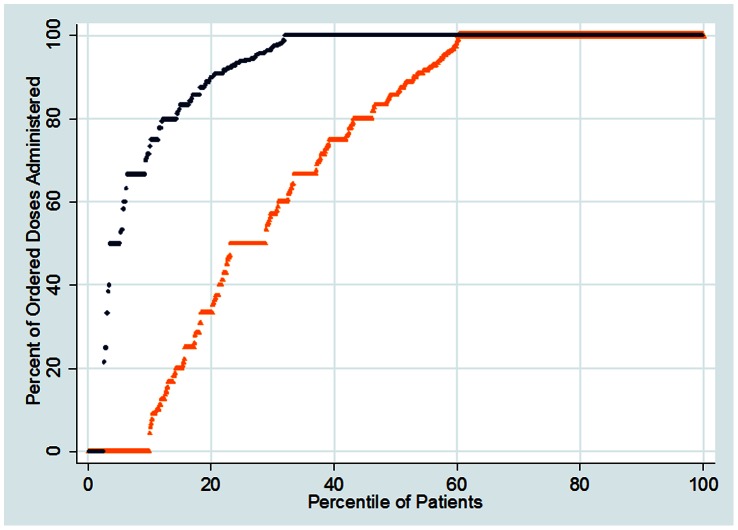
Methods and findings: In this retrospective review of electronic medication administration records, we included adult hospitalized patients who were ordered pharmacologic VTE prophylaxis with unfractionated heparin or enoxaparin over a seven-month period. The primary measure was the proportion of ordered doses of VTE prophylaxis not administered, assessed at the patient, floor, and floor type levels. Differences in non-administration rates between groups were assessed using generalized estimating equations. A total of 103,160 ordered VTE prophylaxis doses during 10,516 patient visits on twenty-nine patient floors were analyzed. Overall, 11.9% of ordered doses were not administered. Approximately 19% of patients missed at least one quarter and 8% of patients missed over one half of ordered doses. There was marked heterogeneity in non-administration rate at the floor level (range: 5-27%). Patients on medicine floors missed a significantly larger proportion (18%) of ordered doses compared to patients on other floor types (8%, Odds Ratio: 2.4, p<0.0001). However, more than half of patients received at least 86% of their ordered doses, even on the lowest performing floor. The 20% of patients who missed at least two ordered doses accounted for 80% of all missed doses.
Conclusions: A substantial proportion of ordered doses of VTE prophylaxis were not administered. The heterogeneity in non-administration rate between patients, floors, and floor types can be used to target interventions. The small proportion of patients that missed multiple ordered doses accounted for a large majority of non-administered doses. This recognition of the Pareto principle provides opportunity to efficiently target a relatively small group of patients for intervention.
Conflict of interest statement
Figures
References
-
- Heit JA (2005) Venous thromboembolism: disease burden, outcomes and risk factors. Journal of Thrombosis and Haemostasis 3(8): 1611–1617. - PubMed
-
- United States Department of Health and Human Services. The Surgeon General’s Call to Action to Prevent Deep Vein Thrombosis and Pulmonary Embolism - 2008. Available: http://www.surgeongeneral.gov/library/calls/deepvein/call-to-action-on-d.... Accessed 13 May 2013. - PubMed
-
- Geerts WH, Pineo GF, Heit JA, Bergqvist D, Lassen MR, et al.. (2004) Prevention of venous thromboembolism: the Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy. Chest 126(3 Suppl): 338S–400S. - PubMed
-
- Anderson AF, Wheeler HB, Goldberg RJ, Hosmer DW, Patwardhan NA, et al. (1991) A population-based perspective of the hospital incidence and case-fatality rates of deep vein thrombosis and pulmonary embolism. The Worcester DVT Study. Arch Int Med 151(5): 933–938. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
