

Preemptive application of airway pressure release ventilation prevents development of acute respiratory distress syndrome in a rat traumatic hemorrhagic shock model
- PMID: 23799354
- PMCID: PMC3780366
- DOI: 10.1097/SHK.0b013e31829efb06
Preemptive application of airway pressure release ventilation prevents development of acute respiratory distress syndrome in a rat traumatic hemorrhagic shock model
Abstract
Background: Once established, the acute respiratory distress syndrome (ARDS) is highly resistant to treatment and retains a high mortality. We hypothesized that preemptive application of airway pressure release ventilation (APRV) in a rat model of trauma/hemorrhagic shock (T/HS) would prevent ARDS.
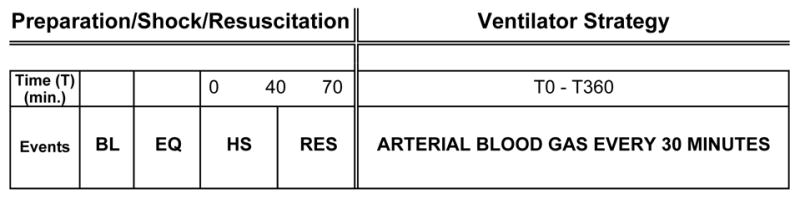
Methods: Rats were anesthetized, instrumented for hemodynamic monitoring, subjected to T/HS, and randomized into two groups: (a) volume cycled ventilation (VC) (n = 5, tidal volume 10 mL/kg; positive end-expiratory pressure 0.5 cmH(2)O) or (b) APRV (n = 4, P(high) = 15-20 cmH(2)O; T(high) = 1.3-1.5 s to achieve 90% of the total cycle time; T(low) = 0.11-0.14 s, which was set to 75% of the peak expiratory flow rate; P(low) = 0 cmH(2)O). Study duration was 6 h.
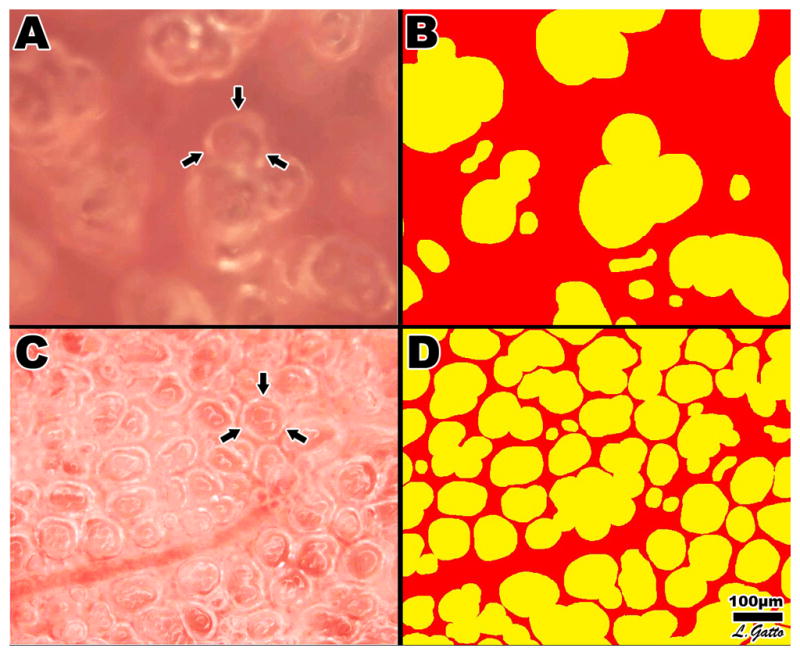
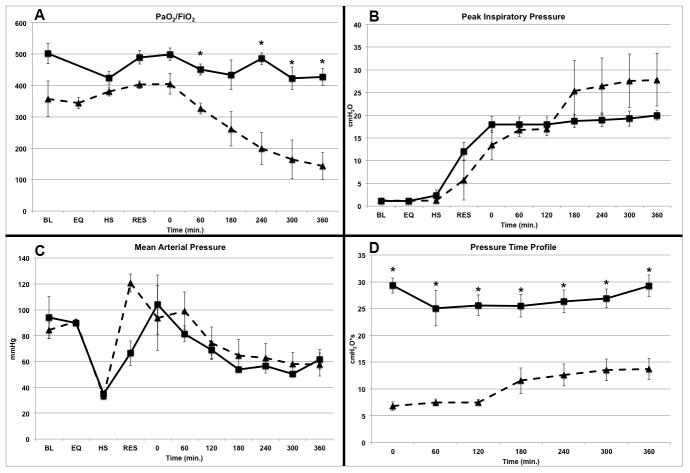
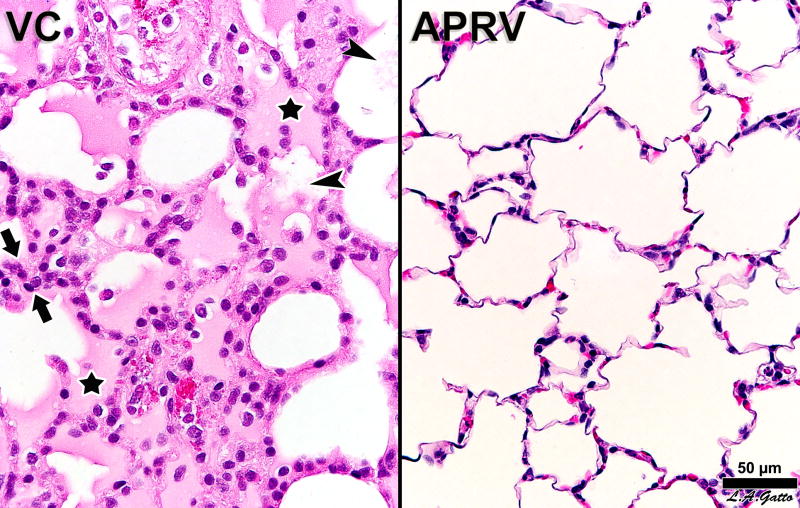
Results: Airway pressure release ventilation prevented lung injury as measured by PaO(2)/FIO(2) (VC 143.3 ± 42.4 vs. APRV 426.8 ± 26.9, P < 0.05), which correlated with a significant decrease in histopathology as compared with the VC group. In addition, APRV resulted in a significant decrease in bronchoalveolar lavage fluid total protein, increased surfactant protein B concentration, and an increase in epithelial cadherin tissue expression. In vivo microscopy demonstrated that APRV significantly improved alveolar patency and stability as compared with the VC group.
Conclusions: Our findings demonstrate that preemptive mechanical ventilation with APRV attenuates the clinical and histologic lung injury associated with T/HS. The mechanism of injury prevention is related to preservation of alveolar epithelial and endothelial integrity. These data support our hypothesis that preemptive APRV, applied using published guidelines, can prevent the development of ARDS.
Conflict of interest statement
There are no conflicts of interest.
Figures
References
-
- Treggiari MM, Hudson LD, Martin DP, Weiss NS, Caldwell E, Rubenfeld G. Effect of acute lung injury and acute respiratory distress syndrome on outcome in critically ill trauma patients. Critical care medicine. 2004;32(2):327–331. - PubMed
-
- Villar J, Blanco J, Anon JM, Santos-Bouza A, Blanch L, Ambros A, Gandia F, Carriedo D, Mosteiro F, Basaldua S, et al. The ALIEN study: incidence and outcome of acute respiratory distress syndrome in the era of lung protective ventilation. Intensive care medicine. 2011;37(12):1932–1941. - PubMed
-
- Cheung AM, Tansey CM, Tomlinson G, Diaz-Granados N, Matte A, Barr A, Mehta S, Mazer CD, Guest CB, Stewart TE, et al. Two-year outcomes, health care use, and costs of survivors of acute respiratory distress syndrome. American journal of respiratory and critical care medicine. 2006;174(5):538–544. - PubMed
-
- Herridge MS, Tansey CM, Matte A, Tomlinson G, Diaz-Granados N, Cooper A, Guest CB, Mazer CD, Mehta S, Stewart TE, et al. Functional disability 5 years after acute respiratory distress syndrome. The New England journal of medicine. 2011;364(14):1293–1304. - PubMed
-
- McIntyre RC, Jr, Pulido EJ, Bensard DD, Shames BD, Abraham E. Thirty years of clinical trials in acute respiratory distress syndrome. Critical care medicine. 2000;28 (9):3314–3331. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
