

National cost of trauma care by payer status
- PMID: 23800441
- PMCID: PMC5995319
- DOI: 10.1016/j.jss.2013.05.068
National cost of trauma care by payer status
Abstract
Background: Several studies have described the burden of trauma care, but few have explored the economic burden of trauma inpatient costs from a payer's perspective or highlighted the differences in the average costs per person by payer status. The present study provides a conservative inpatient national trauma cost estimate and describes the variation in average inpatient trauma cost by payer status.
Methods: A retrospective analysis of patients who had received trauma care at hospitals in the Nationwide Inpatient Sample from 2005-2010 was conducted. Our sample patients were selected using the appropriate "International Classification of Diseases, Ninth Revision, Clinical Modification" codes to identify admissions due to traumatic injury. The data were weighted to provide national population estimates, and all cost and charges were converted to 2010 US dollar equivalents. Generalized linear models were used to describe the costs by payer status, adjusting for patient characteristics, such as age, gender, and race, and hospital characteristics, such as location, teaching status, and patient case mix.
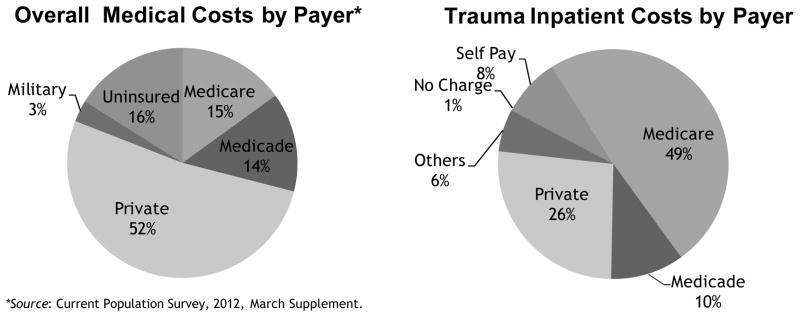
Results: A total of 2,542,551 patients were eligible for the present study, with the payer status as follows: 672,960 patients (26.47%) with private insurance, 1,244,817 (48.96%) with Medicare, 262,256 (10.31%) with Medicaid, 195,056 (7.67%) with self-pay, 18,506 (0.73%) with no charge, and 150,956 (5.94%) with other types of insurance. The estimated yearly trauma inpatient cost burden was highest for Medicare at $17,551,393,082 (46.79%), followed by private insurance ($10,772,025,421 [28.72%]), Medicaid ($3,711,686,012 [9.89%], self-pay ($2,831,438,460 [7.55%]), and other payer types ($2,370,187,494 [6.32%]. The estimated yearly trauma inpatient cost burden was $274,598,190 (0.73%) for patients who were not charged for their inpatient trauma treatment. Our adjusted national inpatient trauma yearly costs were estimated at $37,511,328,659 US dollars. Privately insured patients had a significantly higher mean cost per person than did the Medicare, Medicaid, self-pay, or no charge patients.
Conclusions: The results of the present study have demonstrated that the distribution of trauma burden across payers is significantly different from that of the overall healthcare system and suggest that although the burden of trauma is high, the burden of self-pay or nonreimbursed inpatient services is actually lower than that of overall medical care.
Keywords: Cost of trauma care; Cost shifting by payer; National trauma cost.
Copyright © 2013 Elsevier Inc. All rights reserved.
Figures
References
-
- Murray CJ, Vos T, Lozano R, et al. Disability adjusted life years (DALYs) for 291 diseases and injuries in 21 regions, 1990–2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2013 Dec 15;380(9859):2197–223. - PubMed
-
- WISQARS Leading Causes of Death Reports, 1999–2007. Office of Statistics and Programming, National Center for Injury Prevention and Control, Center for Disease Control and Prevention; [Accessed 1/3/13.]. http://webappa.cdc.gov/sasweb/ncipc/leadcaus10.html.
-
- Shakur H, Robert I, et al. A promise to save 100,000 trauma patients. Lancet. 2013 Dec 15;380(9859):2062–2063. - PubMed
-
- The case for Funding Trauma Research. A Report from the National Trauma Institute. [Accessed 1/3/13.]; http://www.nationaltraumainstitue.org/pdf/case_trauma_funding.pdf.
-
- Soni A. The Five Most Costly Conditions, 2000 and 2004: Estimates for the US Civilian Noninstitutionalized Population. Statistical Brief #167. Agency for Healthcare Research and Quality; Rockville, Md: Mar, 2007. [Accessed 1/3/13]. http://www.meps.ahrq.gov/mepsweb/data_files/publications/st167/stat167.s....
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
