

Cardiac steatosis and left ventricular hypertrophy in patients with generalized lipodystrophy as determined by magnetic resonance spectroscopy and imaging
- PMID: 23800548
- PMCID: PMC3779507
- DOI: 10.1016/j.amjcard.2013.05.036
Cardiac steatosis and left ventricular hypertrophy in patients with generalized lipodystrophy as determined by magnetic resonance spectroscopy and imaging
Abstract
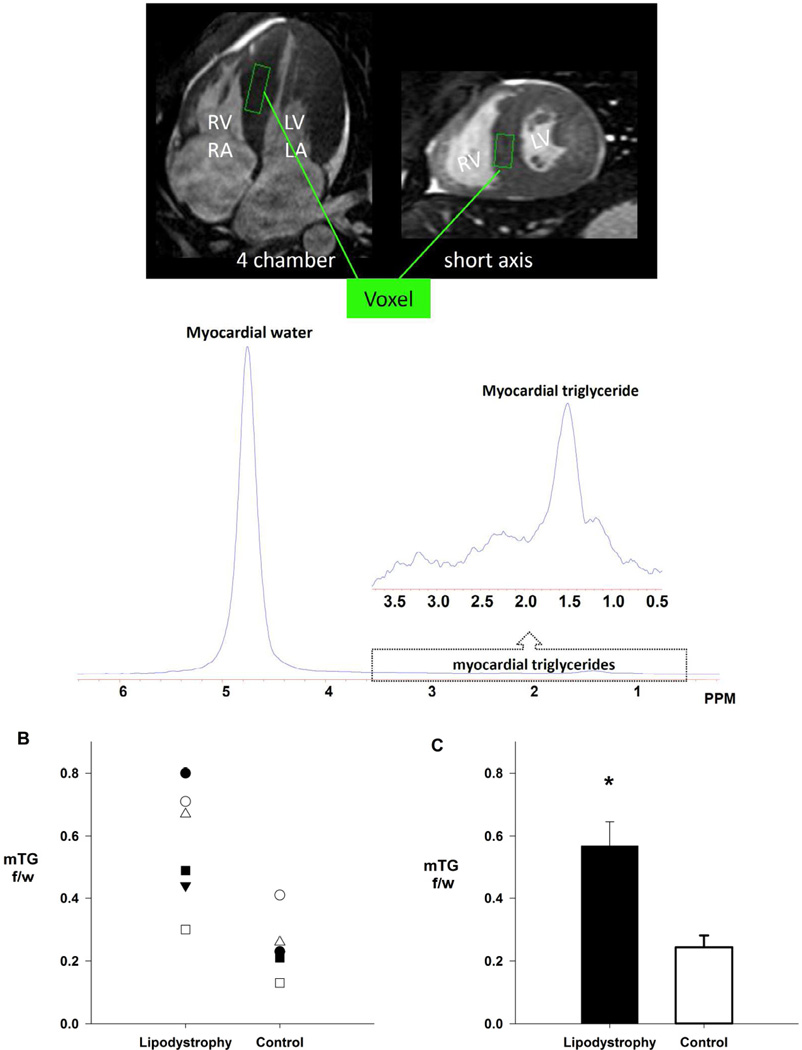
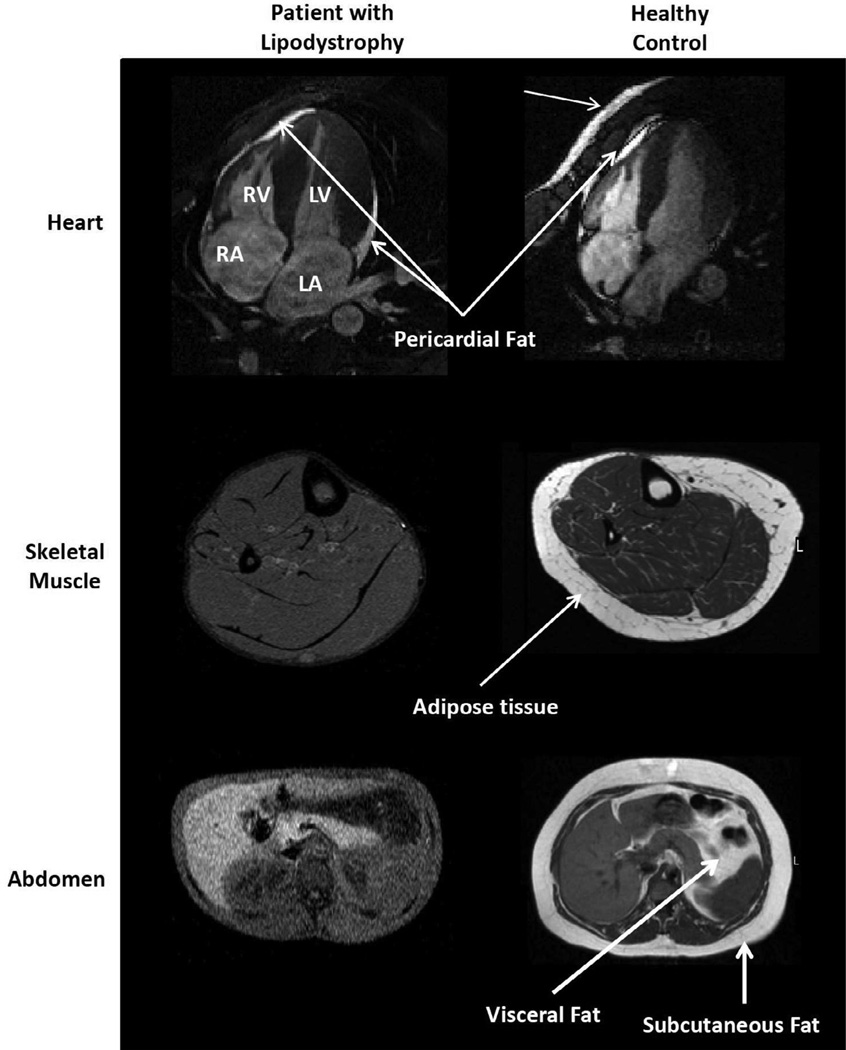
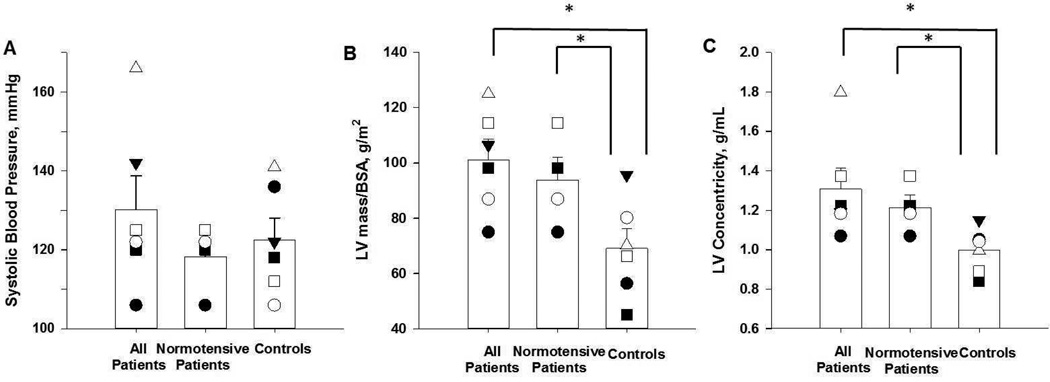
Generalized lipodystrophy is a rare disorder characterized by marked loss of adipose tissue with reduced triglyceride storage capacity, leading to a severe form of metabolic syndrome including hypertriglyceridemia, insulin resistance, type 2 diabetes mellitus, and hepatic steatosis. Recent echocardiographic studies suggest that concentric left ventricular (LV) hypertrophy is another characteristic feature of this syndrome, but the mechanism remains unknown. It has recently been hypothesized that the LV hypertrophy could be an extreme clinical example of "lipotoxic cardiomyopathy": excessive myocyte accumulation of triglyceride leading to adverse hypertrophic signaling. To test this hypothesis, the first cardiac magnetic resonance study of patients with generalized lipodystrophy was performed, using magnetic resonance imaging and localized proton spectroscopy to detect excessive triglyceride content in the hypertrophied myocytes. Six patients with generalized lipodystrophy and 6 healthy controls matched for age, gender, and body mass index were studied. As hypothesized, myocardial triglyceride content was threefold higher in patients than controls: 0.6 ± 0.2% versus 0.2 ± 0.1% (p = 0.004). The presence of pericardial fat was also found, representing a previously undescribed adipose depot in generalized lipodystrophy. Patients with generalized lipodystrophy, compared with controls, also had a striking degree of concentric LV hypertrophy, independent of blood pressure: LV mass index 101.0 ± 18.3 versus 69.0 ± 17.7 g/m(2), respectively (p = 0.02), and LV concentricity 1.3 ± 0.3 versus 0.99 ± 0.1 g/ml, respectively (p = 0.04). In conclusion, these findings advance the lipotoxicity hypothesis as a putative underlying mechanism for the dramatic concentric LV hypertrophy found in generalized lipodystrophy.
Copyright © 2013 The Authors. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures
References
-
- Szczepaniak LS, Babcock EE, Schick F, Dobbins RL, Garg A, Burns DK, McGarry JD, Stein DT. Measurement of intracellular triglyceride stores by H spectroscopy: validation in vivo. Am J Physiol Endocrinol Metab. 1999;276:E977–E989. - PubMed
-
- Simha V, Szczepaniak LS, Wagner AJ, DePaoli AM, Garg A. Effect of Leptin Replacement on Intrahepatic and Intramyocellular Lipid Content in Patients With Generalized Lipodystrophy. Diabetes Care. 2003;26:30–35. - PubMed
-
- Garg A, Misra A. Lipodystrophies: rare disorders causing metabolic syndrome. Endocrinol Metab Clin of North Am. 2004;33:305–331. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
