

Recent advances in the noninvasive diagnosis of renal osteodystrophy
- PMID: 23802194
- PMCID: PMC3805700
- DOI: 10.1038/ki.2013.254
Recent advances in the noninvasive diagnosis of renal osteodystrophy
Abstract
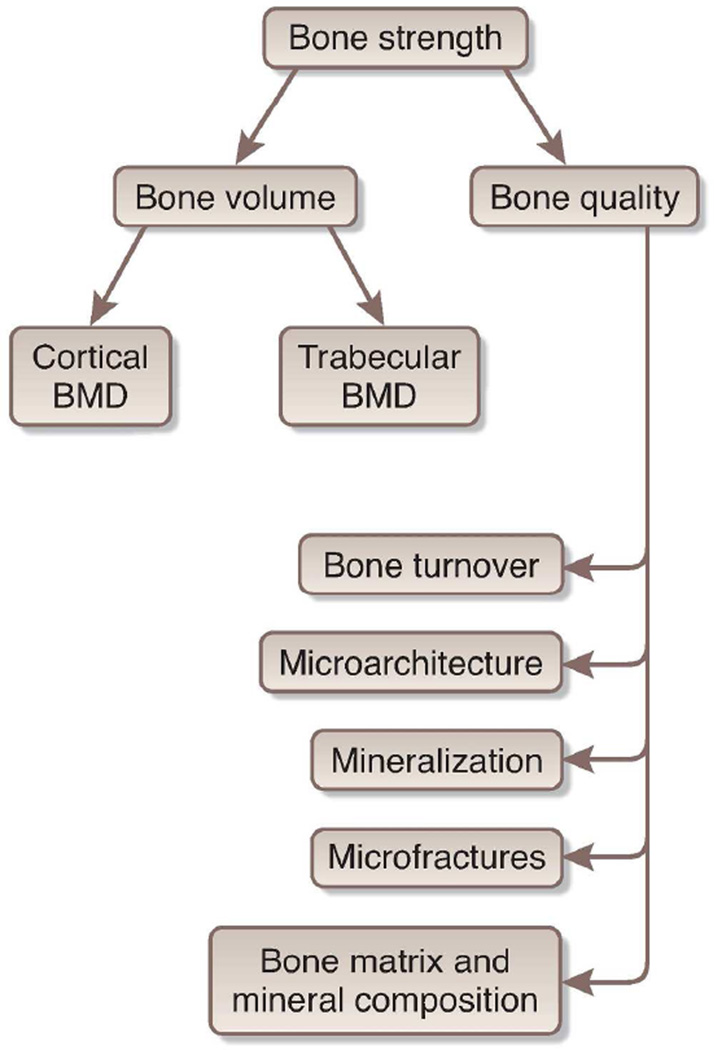
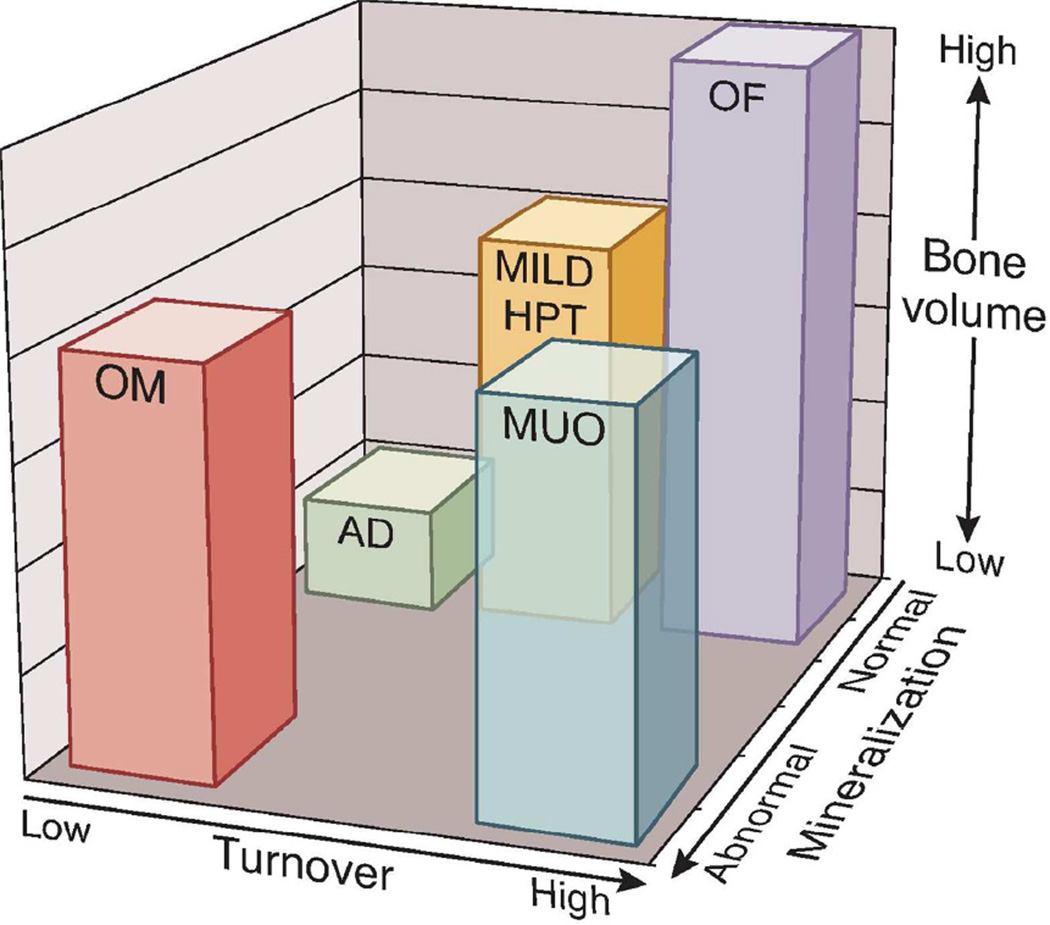
Chronic kidney disease-mineral and bone disorder (CKD-MBD) is the term used to describe a constellation of biochemical abnormalities, bone disturbances that may lead to fractures, and extraskeletal calcification in soft tissues and arteries seen in CKD. This review focuses on the noninvasive diagnosis of renal osteodystrophy, the term used exclusively to define the bone pathology associated with CKD. Transiliac bone biopsy and histomorphometry with double-labeled tetracycline or its derivatives remains the gold standard for diagnosis of renal osteodystrophy. However, histomorphometry provides a 'window' into bone only at a single point in time, and is not clinically practical for studying continuous changes in bone morphology. Furthermore, the etiology of fractures in CKD is multifactorial and not fully explained by histomorphometry findings alone. The propensity of a bone to fracture is determined by bone strength, which is affected by bone mass and bone quality; the latter is a term used to describe the structure and composition of bone. Bone quantity is traditionally assessed by dual X-ray absorptiometry (DXA) and CT-based methods. Bone quality is more difficult to assess noninvasively, but newer techniques are emerging and are described in this review. Ultimately, the optimal diagnostic strategy for renal osteodystrophy may be a combination of multiple imaging techniques and biomarkers that are specific to each gender and race in CKD, with a goal of predicting fracture risk and optimizing therapy.
Figures
References
-
- Lucas RC. On a Form of Late Rickets Associated with Albuminuria. The Lancet. 1883;1(3119):993–994.
-
- Liu SH, Chu HI. Treatment of Renal Osteodystrophy with Dihydrotachysterol (A.T.10) and Iron. Science. 1942;95(2467):388–389. Epub 1942/04/10. - PubMed
-
- Moe S, Drueke T, Cunningham J, Goodman W, Martin K, Olgaard K, et al. Definition, evaluation, and classification of renal osteodystrophy: A position statement from Kidney Disease: Improving Global Outcomes (KDIGO) Kidney international. 2006;69(11):1945–1953. - PubMed
-
- Parfitt AM. Targeted and nontargeted bone remodeling: relationship to basic multicellular unit origination and progression. Bone. 2002;30(1):5–7. - PubMed
-
- Sprague SM. The role of the bone biopsy in the diagnosis of renal osteodystrophy. Semin Dial. 2000;13(3):152–155. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
