

Evaluation of cardiovascular disease burden and therapeutic goal attainment in US adults with chronic kidney disease: an analysis of national health and nutritional examination survey data, 2001-2010
- PMID: 23802885
- PMCID: PMC3701605
- DOI: 10.1186/1471-2369-14-132
Evaluation of cardiovascular disease burden and therapeutic goal attainment in US adults with chronic kidney disease: an analysis of national health and nutritional examination survey data, 2001-2010
Abstract
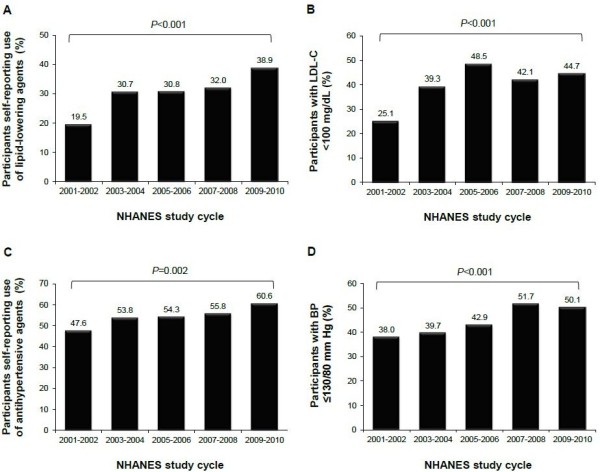
Background: For chronic kidney disease (CKD) patients, national treatment guidelines recommend a low-density lipoprotein cholesterol (LDL-C) goal <100 mg/dL and blood pressure (BP) target <130/80 mmHg. This analysis assessed the current status of cardiovascular (CV) risk factor treatment and control in US adults with CKD.
Methods: Weighted prevalence estimates of CV-related comorbidities, utilization of lipid- and BP-lowering agents, and LDL-C and BP goal attainment in US adults with CKD were assessed among 9,915 men and nonpregnant women aged ≥20 years identified from the fasting subsample of the 2001-2010 National Health and Nutritional Examination Survey (NHANES). Analyses were performed using SAS survey procedures that consider the complex, multistage, probability sampling design of NHANES. All estimates were standardized to the 2008 US adult population (≥20 years). Data were stratified by CKD stage based on presence of albuminuria and estimated glomerular filtration rate (eGFR), calculated using the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) equation. Stage 3 CKD was subdivided into 3a (eGFR 45-59 mL/min/1.73 m(2)) and 3b (eGFR 30-44 mL/min/1.73 m(2)); Stage 5 CKD and dialysis recipients were excluded.
Results: Of the 9,915 NHANES participants identified for analysis, 1,428 had CKD (Stage 1-4), corresponding to a prevalence estimate for US adults aged ≥20 years of 10.2%. Prevalence of CV-related comorbidities increased markedly with CKD stage, with a ~6-12-fold increase in cardiovascular disease, coronary heart disease (CHD), stroke and congestive heart failure between CKD Stage 1 and 4; prevalence of diabetes, hyperlipidemia and hypertension increased by ~1.2-1.6-fold. Use of lipid-lowering agents increased with CKD stage, from 18.1% (Stage 1) to 44.8% (Stage 4). LDL-C goal attainment increased from 35.8% (Stage 1) to 52.8% (Stage 3b), but decreased in Stage 4 (50.7%). BP goal attainment decreased between Stage 1 and 4 (from 49.5% to 30.2%), despite increased use of antihypertensives (from 30.2% to 78.9%).
Conclusions: Individuals with CKD have a high prevalence of CV-related comorbidities. However, attainment of LDL-C or BP goals was low regardless of disease stage. These findings highlight the potential for intensive risk factor modification to maximize CV event reduction in CKD patients at high risk for CHD.
Figures
References
-
- National Kidney Foundation. K/DOQI clinical practice guidelines for chronic kidney disease: evaluation, classification, and stratification. Am J Kidney Dis. 2002;39(2 Suppl 1):S1–S266. - PubMed
-
- Kidney Disease. KDIGO 2012 clinical practice guideline for the evaluation and management of chronic kidney disease. Kidney Int Suppl. 2013;3(1):1–150. - PubMed
-
- Sarnak MJ, Levey AS. Cardiovascular disease and chronic renal disease: a new paradigm. Am J Kidney Dis. 2000;35(4 Suppl 1):S117–S131. - PubMed
-
- Sarnak MJ, Levey AS, Schoolwerth AC, Coresh J, Culleton B, Hamm LL, McCullough PA, Kasiske BL, Kelepouris E, Klag MJ, Parfrey P, Pfeffer M, Raij L, Spinosa DJ, Wilson PW. Kidney disease as a risk factor for development of cardiovascular disease: a statement from the american heart association councils on kidney in cardiovascular disease, high blood pressure research, clinical cardiology, and epidemiology and prevention. Circulation. 2003;108(17):2154–2169. doi: 10.1161/01.CIR.0000095676.90936.80. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
