

Review
doi: 10.4103/0301-4738.114103.
Surgical management in patient with uveitis
Affiliations
- PMID: 23803480
- PMCID: PMC3744781
- DOI: 10.4103/0301-4738.114103
Item in Clipboard
Review
Surgical management in patient with uveitis
Indian J Ophthalmol.
2013 Jun.
Abstract
Surgery in the management of uveitis can be divided based on indication: either for therapeutic or can be for diagnostic purposes or to manage complications. The commonest indications include: Visual rehabilitation: surgery for removal of cataract, band keratopathy, corneal scars, pupillary membranes, removal of dense vitreous membranes, management of complications: anti-glaucoma surgery, vitreous hemorrhage, retinal detachment and chronic hypotony and diagnostic: aqueous tap, vitreous biopsy, tissue biopsy (iris, choroid). In this review, we shall describe the surgical technique for visual rehabilitation and for management of complications.
Conflict of interest statement
Figures
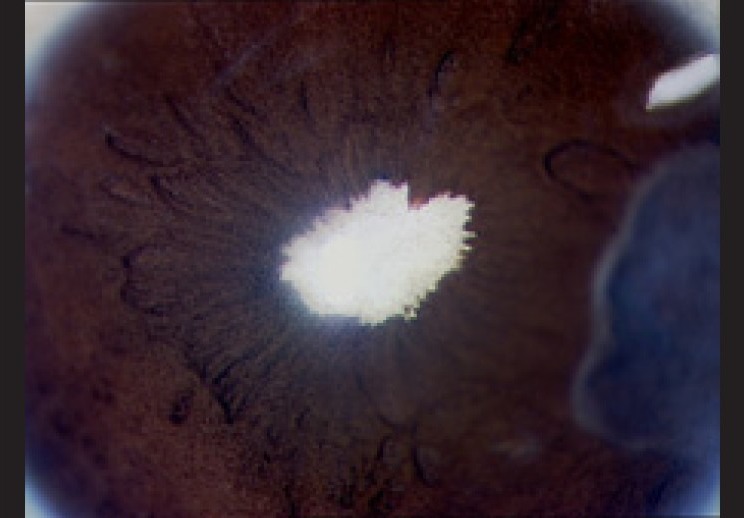
Slit lamp photograph shows a patient with chronic idiopathic panuveitis with a white cataract and extensive posterior synechiae and neo-vascularization on the anterior lens capsule

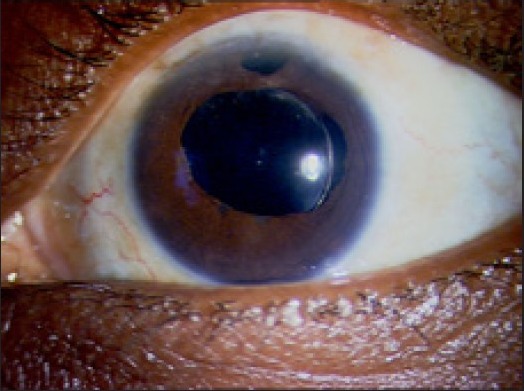
Complicated cataract in a patient with idiopathic anterior uveitis with posterior synechia and a quiet eye at the time of surgery
Post-operative outcome after phacoemulsification

Pre-operative (a) photograph of a patient with Fuch's uveitic syndrome, showing diffuse, large keratic precipitates

Post-operative photograph shows recurrence of these precipitates as stellate deposits on the intraocular lens

Optic capture of the intraocular lens, which was implanted in the sulcus and pupillary membranes in a 35-year-old female patient with intermediate uveitis who underwent surgery 5 years ago

(a and b) Slit lamp photograph of a patient with chronic uveitis and secondary glaucoma who underwent Ahmed glaucoma valve implant, showing the valve well positioned in the anterior chamber, diffuse (a) and slit illumination (b)

Intra-operative photograph showing single port diagnostic vitrectomy using 23 G vitrectomy cutter with 2 ml disposable syringe connected to suction tubing
Similar articles
-
Surgical treatment of uveitis.Coll Antropol. 2001;25 Suppl:71-6. Coll Antropol. 2001. PMID: 11817019
-
Surgical approaches to uveitis.Int Ophthalmol Clin. 1990 Fall;30(4):314-7. doi: 10.1097/00004397-199030040-00023. Int Ophthalmol Clin. 1990. PMID: 2228481 Review. No abstract available.
-
[Surgical treatment of secondary glaucoma in uveitis with extremely shallow anterior chamber and cataract].Yan Ke Xue Bao. 2007 Dec;23(4):238-42. Yan Ke Xue Bao. 2007. PMID: 18303673 Chinese.
-
Uveitis: effect of vitrectomy combined with lensectomy.Ophthalmology. 1979 Jul;86(7):1320-9. doi: 10.1016/s0161-6420(79)35395-7. Ophthalmology. 1979. PMID: 233864
-
Combined extracapsular cataract extraction, posterior chamber intraocular lens implantation, and pars plana vitrectomy.Ophthalmic Surg. 1993 Jul;24(7):446-52. Ophthalmic Surg. 1993. PMID: 8351090 Review.
Cited by
-
Phacoemulsification versus small incision cataract surgery in patients with uveitis.Int J Ophthalmol. 2015 Oct 18;8(5):965-70. doi: 10.3980/j.issn.2222-3959.2015.05.20. eCollection 2015. Int J Ophthalmol. 2015. PMID: 26558210 Free PMC article.
-
Goniotomy for Non-Infectious Uveitic Glaucoma in Children.J Clin Med. 2023 Mar 12;12(6):2200. doi: 10.3390/jcm12062200. J Clin Med. 2023. PMID: 36983202 Free PMC article.
-
Surgical Management in a Patient With Complex Uveitic Glaucoma: A Case Report.Medicine (Baltimore). 2015 Aug;94(31):e1248. doi: 10.1097/MD.0000000000001248. Medicine (Baltimore). 2015. PMID: 26252285 Free PMC article.
-
Pars plana vitrectomy in uveitis in the era of microincision vitreous surgery.Indian J Ophthalmol. 2020 Sep;68(9):1844-1851. doi: 10.4103/ijo.IJO_1625_20. Indian J Ophthalmol. 2020. PMID: 32823401 Free PMC article. Review.
-
[Pharmacological treatment strategies and surgical options for uveitis].Ophthalmologe. 2019 Oct;116(10):942-950. doi: 10.1007/s00347-019-0870-x. Ophthalmologe. 2019. PMID: 30796601 Review. German.
References
-
- Foster CS, Rashid S. Management of coincident cataract and uveitis. Curr Opin Ophthalmol. 2003;14:1–6. - PubMed
-
- Hazari A, Sangwan VS. Cataract surgery in uveitis. Indian J Ophthalmol. 2002;50:103–7. - PubMed
-
- Javadi MA, Jafarinasab MR, Araghi AA, Mohammadpour M, Yazdani S. Outcomes of phacoemulsification and in-the-bag intraocular lens implantation in Fuchs’ heterochromic iridocyclitis. J Cataract Refract Surg. 2005;31:997–1001. - PubMed
-
- Harper SL, Foster CS. Intraocular lens explantation in uveitis. Int Ophthalmol Clin. 2000;40:107–16. - PubMed
-
- Ganesh SK, Babu K, Biswas J. Phacoemulsification with intraocular lens implantation in cases of pars planitis. J Cataract Refract Surg. 2004;30:2072–6. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
