

A novel risk-adjusted nomogram for rectal cancer surgery outcomes
- PMID: 23803722
- PMCID: PMC3947615
- DOI: 10.1001/jamasurg.2013.2136
A novel risk-adjusted nomogram for rectal cancer surgery outcomes
Abstract
Importance: The circumferential resection margin is the primary determinant of local recurrence and a major factor in survival in rectal cancer. Neither chemotherapy nor chemoradiation compensates for a margin positive for cancer.
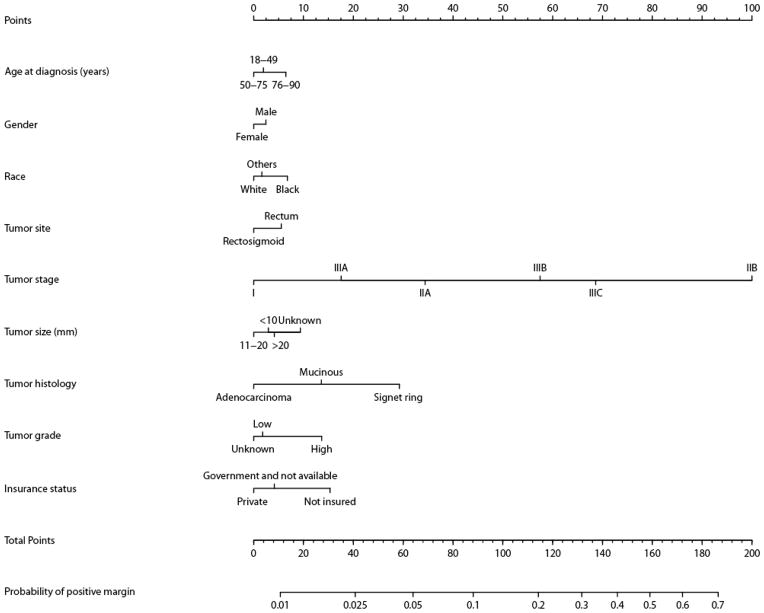
Objective: To identify treatment-related factors associated with hospital margin-positive resection and to develop a tool that could be used by individual hospitals to assess their outcomes based on their unique mix of patient and tumor characteristics.
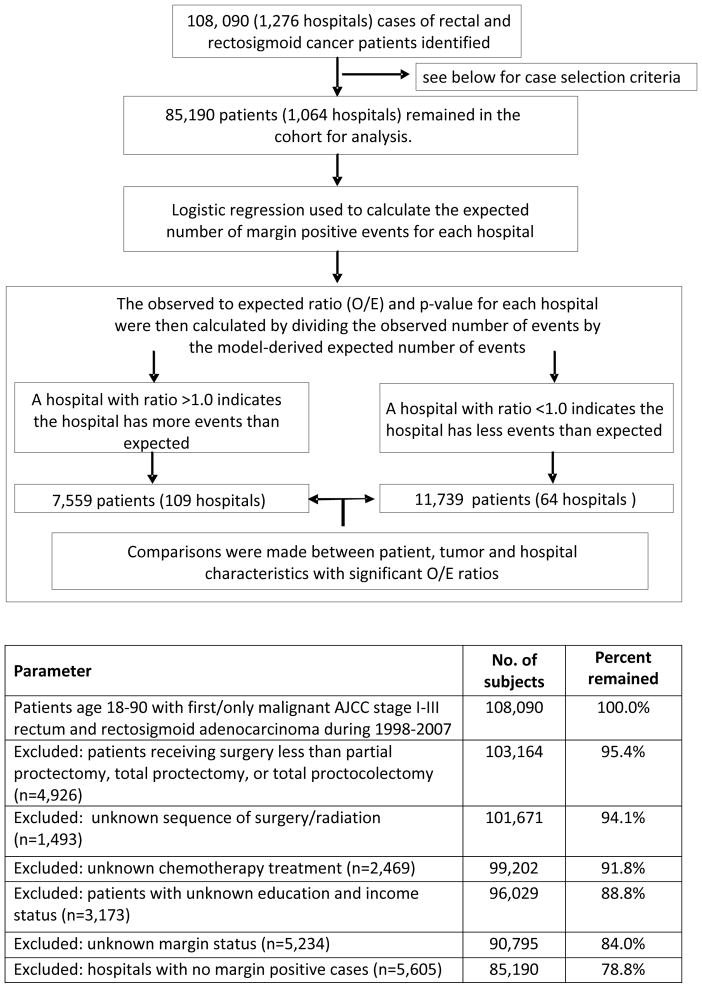
Design: Retrospective review of the National Cancer Data Base, 1998-2007.
Settings: Community and academic/research hospitals.
Participants: Individuals with histologically confirmed localized rectal/rectosigmoid adenocarcinoma.
Exposure: All individuals underwent radical resection for rectal cancer with or without neoadjuvant therapy.
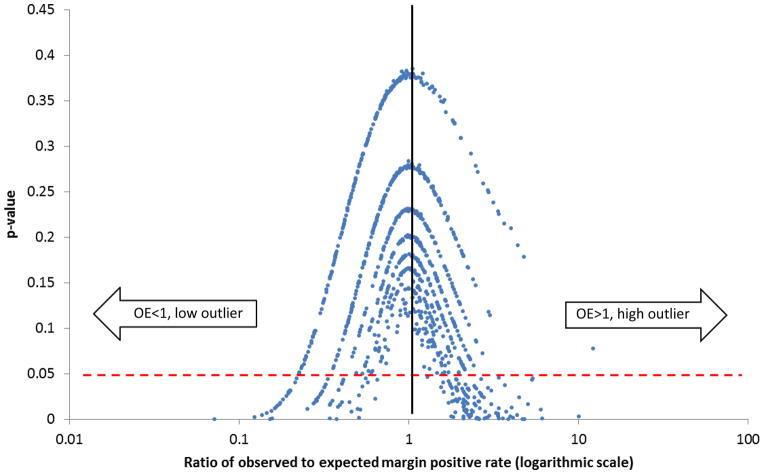
Main outcomes and measures: Rate of margin positivity determined and adjusted for patient- and tumor-related factors to calculate expected margin positivity per hospital. An observed to expected ratio was calculated based on patient- and tumor-related factors to identify treatment-associated variation.
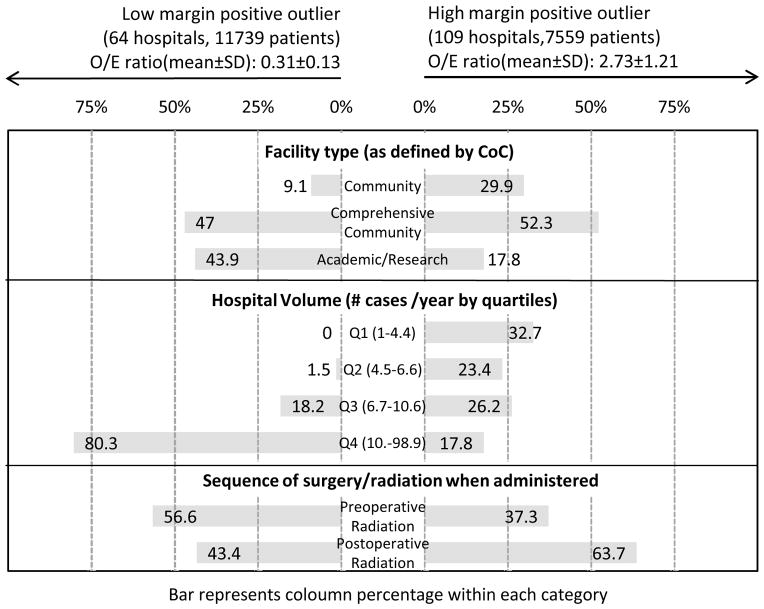
Results: The overall margin-positive resection rate was 5.2%. Patients with margins positive for cancer were more likely to be older, male, and African American; not have private insurance; and have their cancer diagnosed later in the study period. Associated tumor-related factors include rectal location, higher American Joint Committee on Cancer stage, signet/mucinous histology, and poor/undifferentiated grade. Among hospitals that were significantly low outliers, 47% were comprehensive community hospitals, and 43.9% were academic/research hospitals; of those that were significantly high outliers, 52.3% were comprehensive community hospitals, and 17.8% were academic/research hospitals. High-volume centers made up 80% of significantly low outlier hospitals and 17% of significantly high outlier hospitals. The rates of chemotherapy and radiation were similar, but low outlier hospitals gave more neoadjuvant radiation (26.3% vs 17%).
Conclusions and relevance: After adjustment for patient- and tumor-related factors, we identified both low and high outlier hospitals for margin positivity at resection, as well as potentially modifiable risk factors. The nomogram created in this model allows for the evaluation of observed and expected event rates for individual hospitals, providing a hospital self-assessment tool for identifying targets for improvement.
Figures
Comment in
-
Multidisciplinary treatment of rectal cancer: the way of the future.JAMA Surg. 2013 Aug;148(8):778. doi: 10.1001/jamasurg.2013.2151. JAMA Surg. 2013. PMID: 23803771 No abstract available.
References
-
- Siegel R, Naishadham D, Jemal A. Cancer statistics, 2012. CA Cancer J Clin. 2012 Jan-Feb;62(1):10–29. - PubMed
-
- McCall JL, Cox MR, Wattchow DA. Analysis of local recurrence rates after surgery alone for rectal cancer. Int J Colorectal Dis. 1995;10(3):126–132. - PubMed
-
- Martling AL, Holm T, Rutqvist LE, Moran BJ, Heald RJ, Cedemark B. Effect of a surgical training programme on outcome of rectal cancer in the County of Stockholm. Stockholm Colorectal Cancer Study Group, Basingstoke Bowel Cancer Research Project. Lancet. 2000 Jul 8;356(9224):93–96. - PubMed
-
- Adam IJ, Mohamdee MO, Martin IG, et al. Role of circumferential margin involvement in the local recurrence of rectal cancer. Lancet. 1994 Sep 10;344(8924):707–711. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
