

National trends in hospital-acquired preventable adverse events after major cancer surgery in the USA
- PMID: 23804313
- PMCID: PMC3696870
- DOI: 10.1136/bmjopen-2013-002843
National trends in hospital-acquired preventable adverse events after major cancer surgery in the USA
Abstract
Objectives: While multiple studies have demonstrated variations in the quality of cancer care in the USA, payers are increasingly assessing structure-level and process-level measures to promote quality improvement. Hospital-acquired adverse events are one such measure and we examine their national trends after major cancer surgery.
Design: Retrospective, cross-sectional analysis of a weighted-national estimate from the Nationwide Inpatient Sample (NIS) undergoing major oncological procedures (colectomy, cystectomy, oesophagectomy, gastrectomy, hysterectomy, lung resection, pancreatectomy and prostatectomy). The Agency for Healthcare Research and Quality Patient Safety Indicators (PSIs) were utilised to identify trends in hospital-acquired adverse events.
Setting: Secondary and tertiary care, US hospitals in NIS PARTICIPANTS: A weighted-national estimate of 2 508 917 patients (>18 years, 1999-2009) from NIS.
Primary outcome measures: Hospital-acquired adverse events.
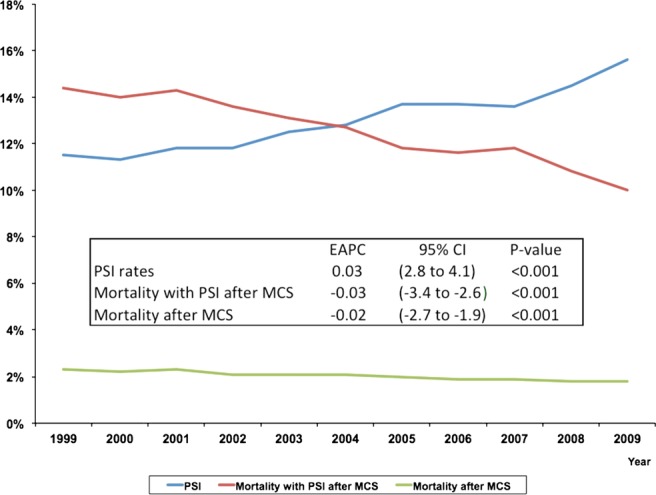
Results: 324 852 patients experienced ≥1-PSI event (12.9%). Patients with ≥1-PSI experienced higher rates of in-hospital mortality (OR 19.38, 95% CI 18.44 to 20.37), prolonged length of stay (OR 4.43, 95% CI 4.31 to 4.54) and excessive hospital-charges (OR 5.21, 95% CI 5.10 to 5.32). Patients treated at lower volume hospitals experienced both higher PSI events and failure-to-rescue rates. While a steady increase in the frequency of PSI events after major cancer surgery has occurred over the last 10 years (estimated annual % change (EAPC): 3.5%, p<0.001), a concomitant decrease in failure-to-rescue rates (EAPC -3.01%) and overall mortality (EAPC -2.30%) was noted (all p<0.001).
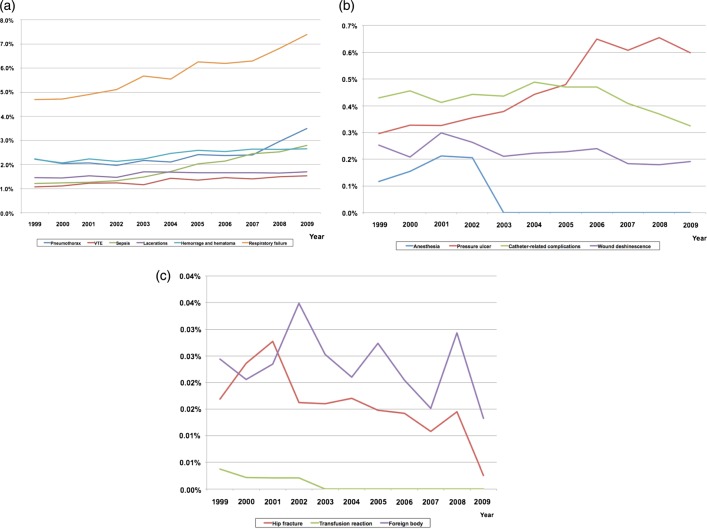
Conclusions: Over the past decade, there has been a substantial increase in the national frequency of potentially avoidable adverse events after major cancer surgery, with a detrimental effect on numerous outcome-level measures. However, there was a concomitant reduction in failure-to-rescue rates and overall mortality rates. Policy changes to improve the increasing burden of specific adverse events, such as postoperative sepsis, pressure ulcers and respiratory failure, are required.
Keywords: Cancer surgery; Patient Safety Indicators; Preventable Adverse Events; Quality Improvement.
Figures
References
-
- Iezzoni LI, Foley SM, Heeren T, et al. A method for screening the quality of hospital care using administrative data: preliminary validation results. Qual Rev Bull 1992;18:361–71 - PubMed
-
- http://www.qualityindicators.ahrq.gov/modules/psi_resources.aspx (accessed 9 Sep 2012)
-
- Zhan C, Miller MR. Excess length of stay, charges, and mortality attributable to medical injuries during hospitalization. JAMA 2003;290:1868–74 - PubMed
-
- Siegel R, Naishadham D, Jemal A. Cancer statistics, 2012. CA Cancer J Clin 2012;62:10–29 - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous