

Is it time for a new paradigm for systemic cancer treatment? Lessons from a century of cancer chemotherapy
- PMID: 23805101
- PMCID: PMC3691519
- DOI: 10.3389/fphar.2013.00068
Is it time for a new paradigm for systemic cancer treatment? Lessons from a century of cancer chemotherapy
Abstract
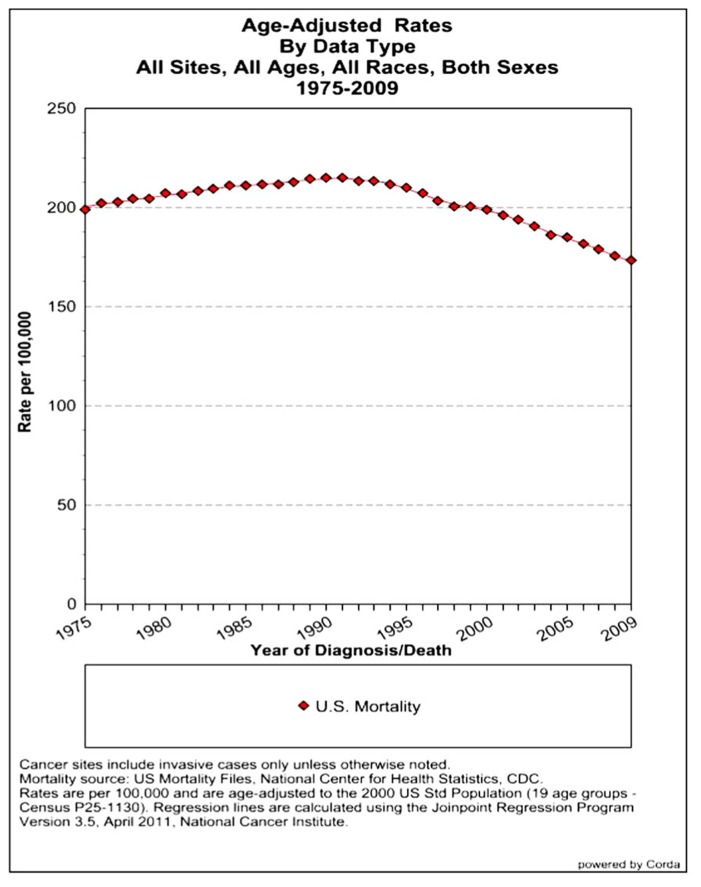
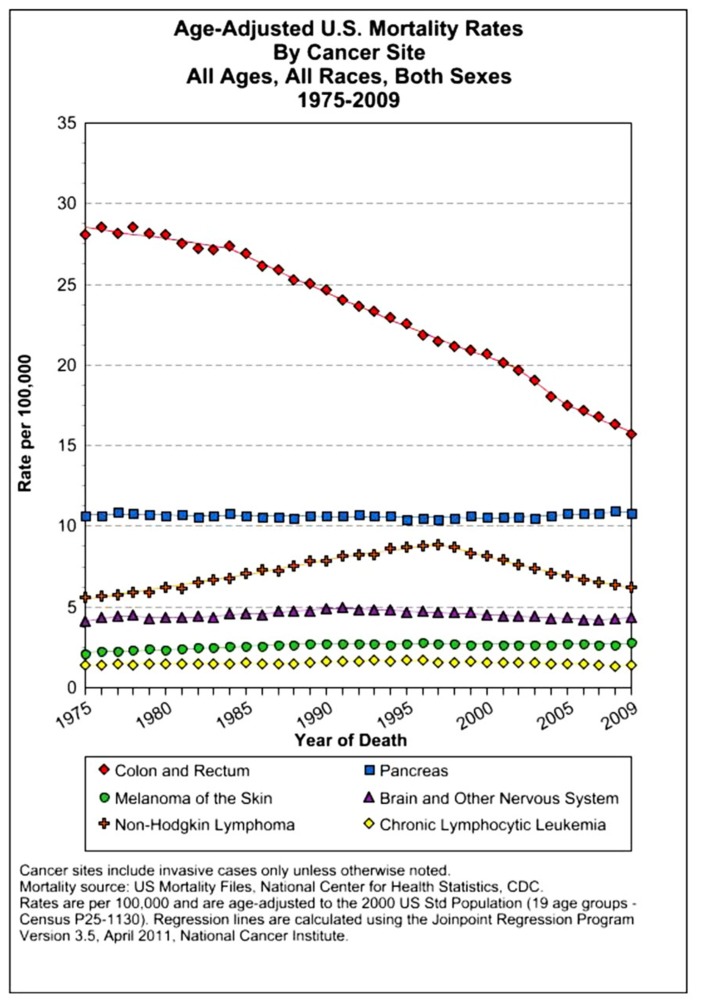
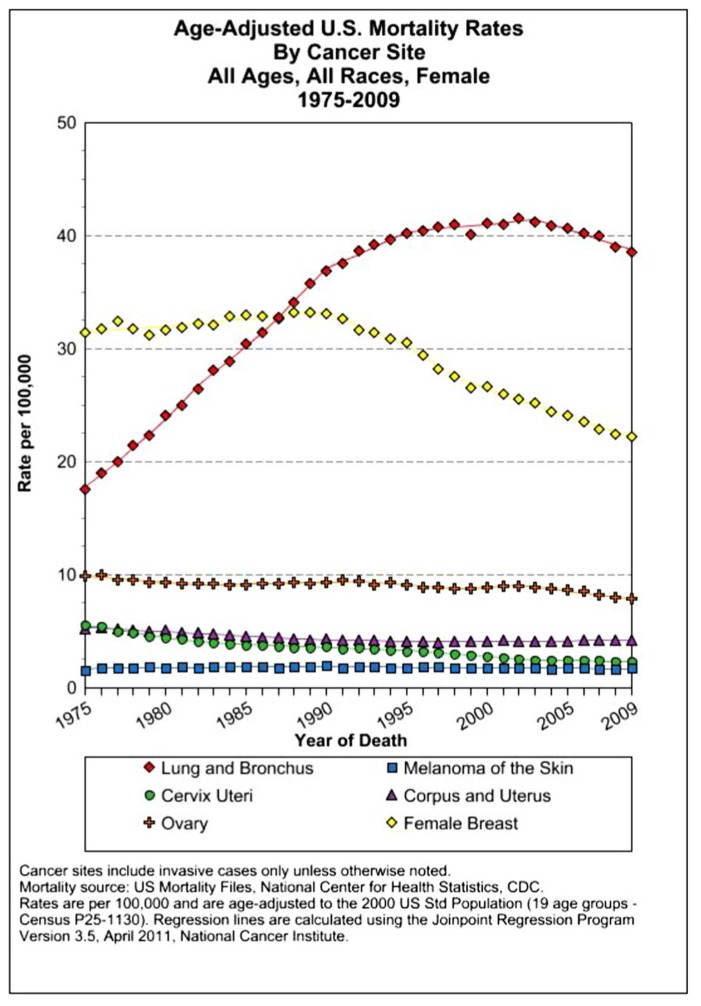
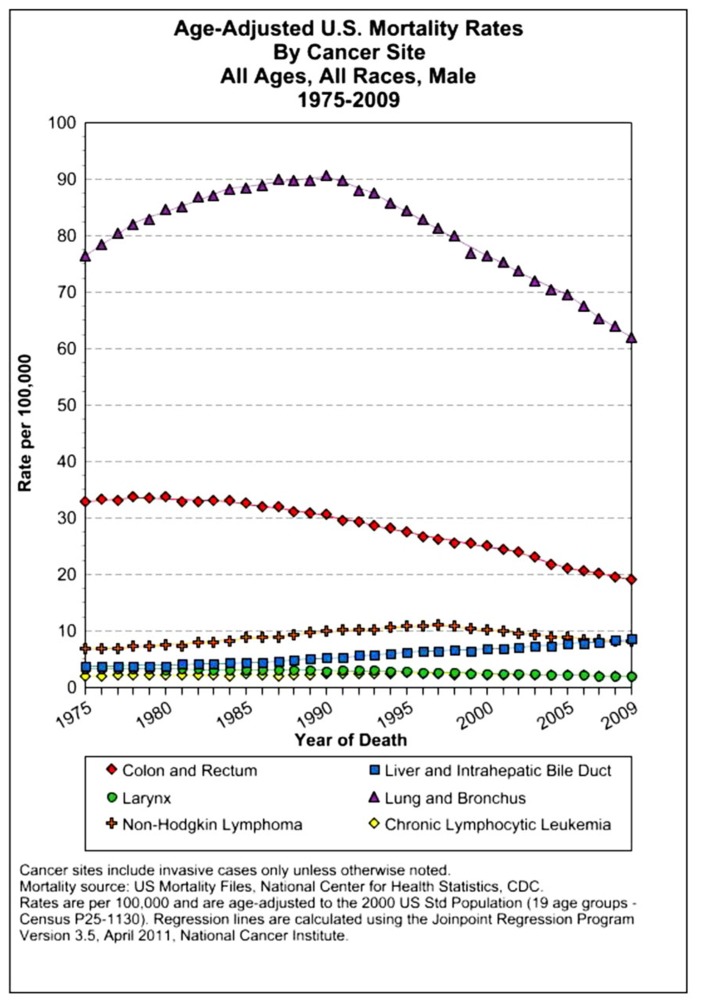
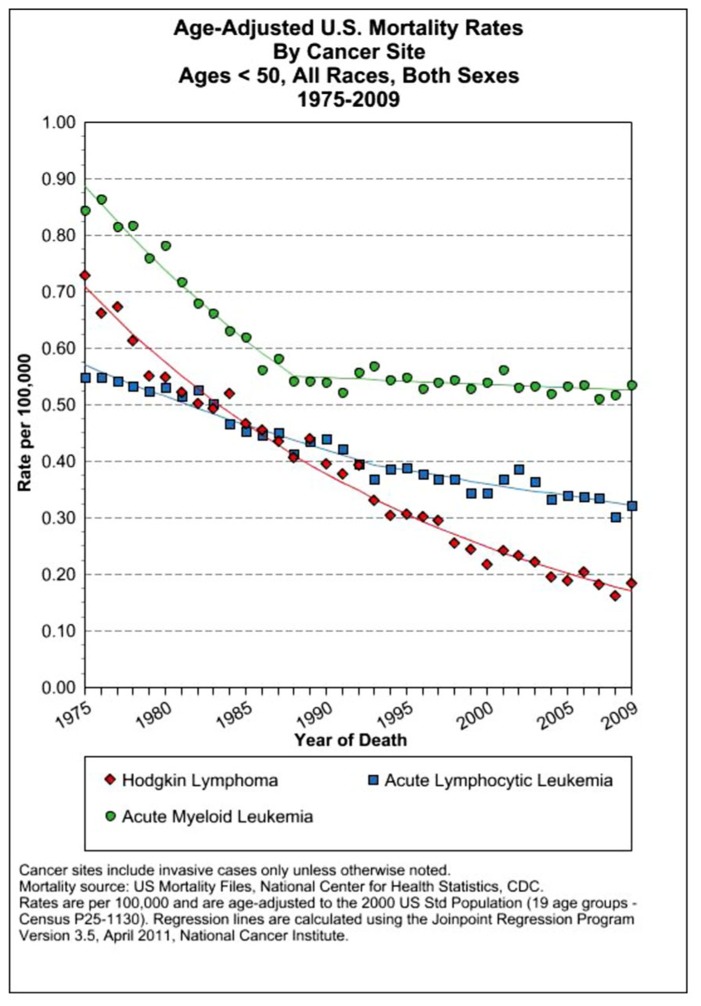
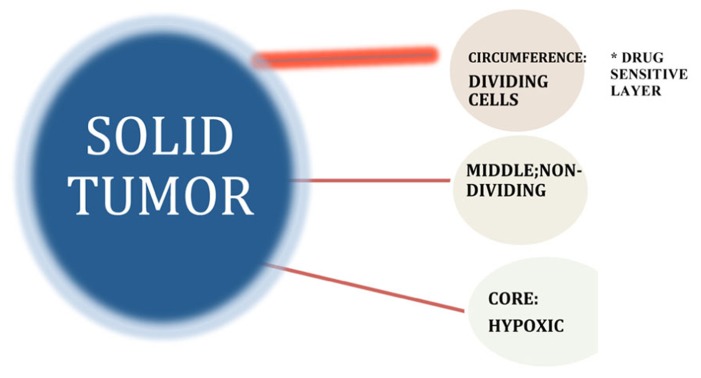
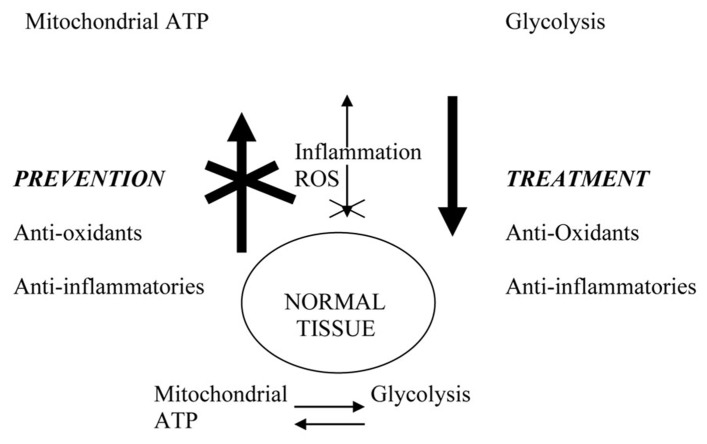
U.S. SEER (Surveillance Epidemiology and End Results) data for age-adjusted mortality rates for all cancers combined for all races show only a modest overall 13% decline over the past 35 years. Moreover, the greatest contributor to cancer mortality is treatment-resistant metastatic disease. The accepted therapeutic paradigm for the past half-century for the treatment of advanced cancers has involved the use of systemic chemotherapy drugs cytotoxic for cycling cells (both normal and malignant) during DNA synthesis and/or mitosis. The failure of this therapeutic modality to achieve high-level, consistent rates of disease-free survival for some of the most common cancers, including tumors of the lung, colon breast, brain, melanoma, and others is the focus of this paper. A retrospective assessment of critical milestones in cancer chemotherapy indicates that most successful therapeutic regimens use cytotoxic cell cycle inhibitors in combined, maximum tolerated, dose-dense acute treatment regimens originally developed to treat acute lymphoblastic leukemia and some lymphomas. Early clinical successes in this area led to their wholesale application to the treatment of solid tumor malignancies that, unfortunately, has not produced consistent, long-term high cure rates for many common cancers. Important differences in therapeutic sensitivity of leukemias/lymphomas versus solid tumors can be explained by key biological differences that define the treatment-resistant solid tumor phenotype. A review of these clinical outcome data in the context of recent developments in our understanding of drug resistance mechanisms characteristic of solid tumors suggests the need for a new paradigm for the treatment of chemotherapy-resistant cancers. In contrast to reductionist approaches, the systemic approach targets both microenvironmental and systemic factors that drive and sustain tumor progression. These systemic factors include dysregulated inflammatory and oxidation pathways shown to be directly implicated in the development and maintenance of the cancer phenotype. The paradigm stresses the importance of a combined preventive/therapeutic approach involving adjuvant chemotherapies that incorporate anti-inflammatory and anti-oxidant therapeutics.
Keywords: adjuvant; anti-inflammatory; anti-oxidant; chemotherapy; drug resistance; neoplasm; tumor microenvironment.
Figures

Similar articles
-
Overview of resistance to systemic therapy in patients with breast cancer.Adv Exp Med Biol. 2007;608:1-22. doi: 10.1007/978-0-387-74039-3_1. Adv Exp Med Biol. 2007. PMID: 17993229 Review.
-
The Goal of Cancer Treatment.Oncologist. 1998;3(4):V. Oncologist. 1998. PMID: 10388118
-
Anti-inflammatory/antioxidant use in long-term maintenance cancer therapy: a new therapeutic approach to disease progression and recurrence.Ther Adv Med Oncol. 2014 Mar;6(2):52-68. doi: 10.1177/1758834014521111. Ther Adv Med Oncol. 2014. PMID: 24587831 Free PMC article. Review.
-
Cancer Drug Development: New Targets for Cancer Treatment.Oncologist. 1996;1(3):II-III. Oncologist. 1996. PMID: 10387987
-
The Challenge of Developing New Therapies for Childhood Cancers.Oncologist. 1997;2(1):I-II. Oncologist. 1997. PMID: 10388032
Cited by
-
Machine Learning: A New Prospect in Multi-Omics Data Analysis of Cancer.Front Genet. 2022 Jan 27;13:824451. doi: 10.3389/fgene.2022.824451. eCollection 2022. Front Genet. 2022. PMID: 35154283 Free PMC article. Review.
-
Spatial Heterogeneity and Evolutionary Dynamics Modulate Time to Recurrence in Continuous and Adaptive Cancer Therapies.Cancer Res. 2018 Apr 15;78(8):2127-2139. doi: 10.1158/0008-5472.CAN-17-2649. Epub 2018 Jan 30. Cancer Res. 2018. PMID: 29382708 Free PMC article.
-
Tumour-targeting bacteria-based cancer therapies for increased specificity and improved outcome.Microb Biotechnol. 2017 Sep;10(5):1074-1078. doi: 10.1111/1751-7915.12787. Epub 2017 Aug 3. Microb Biotechnol. 2017. PMID: 28771926 Free PMC article. Review.
-
Bacteria in Cancer Therapy: Renaissance of an Old Concept.Int J Microbiol. 2016;2016:8451728. doi: 10.1155/2016/8451728. Epub 2016 Mar 8. Int J Microbiol. 2016. PMID: 27051423 Free PMC article. Review.
-
Ubc13: the Lys63 ubiquitin chain building machine.Oncotarget. 2016 Sep 27;7(39):64471-64504. doi: 10.18632/oncotarget.10948. Oncotarget. 2016. PMID: 27486774 Free PMC article. Review.
References
-
- Anderson W. F., Umar A., Viner J. L., Hawk E. T. (2002)The role of cyclooxygenase inhibitors in cancer prevention. Curr. Pharm. Des. 1035–1062 - PubMed
-
- Annemijn M., Algra B., Rothwell P. (2012) Effects of regular aspirin on long-term cancer incidence and metastasis: a systematic comparison of evidence from observational studies versus randomised trials. Lancet 13 518–527 - PubMed
-
- Au J. L., Jang S. H., Wientjes M. G. (2002) Clinical aspects of drug delivery to tumors. J. Control Release 78 81–95 - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous