

Control of hypertension in the critically ill: a pathophysiological approach
- PMID: 23806076
- PMCID: PMC3704960
- DOI: 10.1186/2110-5820-3-17
Control of hypertension in the critically ill: a pathophysiological approach
Abstract
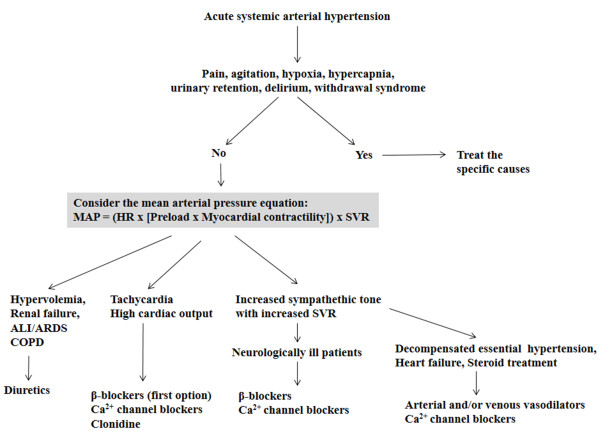
Severe acute arterial hypertension can be associated with significant morbidity and mortality. After excluding a reversible etiology, choice of therapeutic intervention should be based on evaluation of a number of factors, such as age, comorbidities, and other ongoing therapies. A rational pathophysiological approach should then be applied that integrates the effects of the drug on blood volume, vascular tone, and other determinants of cardiac output. Vasodilators, calcium channel blockers, and beta-blocking agents can all decrease arterial pressure but by totally different modes of action, which may be appropriate or contraindicated in individual patients. There is no preferred agent for all situations, although some drugs may have a more attractive profile than others, with rapid onset action, short half-life, and fewer adverse reactions. In this review, we focus on the main mechanisms underlying severe hypertension in the critically ill and how using a pathophysiological approach can help the intensivist decide on treatment options.
Figures
References
-
- Chobanian AV, Bakris GL, Black HR, Cushman WC, Green LA, Izzo JL Jr, Jones DW, Materson BJ, Oparil S, Wright JT Jr, Roccella EJ. The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure: the JNC 7 report. JAMA. 2003;3:2560–2572. doi: 10.1001/jama.289.19.2560. - DOI - PubMed
-
- Rosamond W, Flegal K, Furie K, Go A, Greenlund K, Haase N, Hailpern SM, Ho M, Howard V, Kissela B, Kittner S, Lloyd-Jones D, McDermott M, Meigs J, Moy C, Nichol G, O'Donnell C, Roger V, Sorlie P, Steinberger J, Thom T, Wilson M, Hong Y. Heart disease and stroke statistics–2008 update: a report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation. 2008;3:e25–e146. - PubMed
-
- Shafi T. Hypertensive urgencies and emergencies. Ethn Dis. 2004;3:S2–S7. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
