

The effect of microvascular obstruction and intramyocardial hemorrhage on contractile recovery in reperfused myocardial infarction: insights from cardiovascular magnetic resonance
- PMID: 23806080
- PMCID: PMC3707770
- DOI: 10.1186/1532-429X-15-58
The effect of microvascular obstruction and intramyocardial hemorrhage on contractile recovery in reperfused myocardial infarction: insights from cardiovascular magnetic resonance
Abstract
Background: Following acute myocardial infarction (AMI), microvascular obstruction (MO) and intramyocardial hemorrhage (IMH) adversely affect left ventricular remodeling and prognosis independently of infarct size. Whether this is due to infarct zone remodeling, changes in remote myocardium or other factors is unknown. We investigated the role of MO and IMH in recovery of contractility in infarct and remote myocardium.
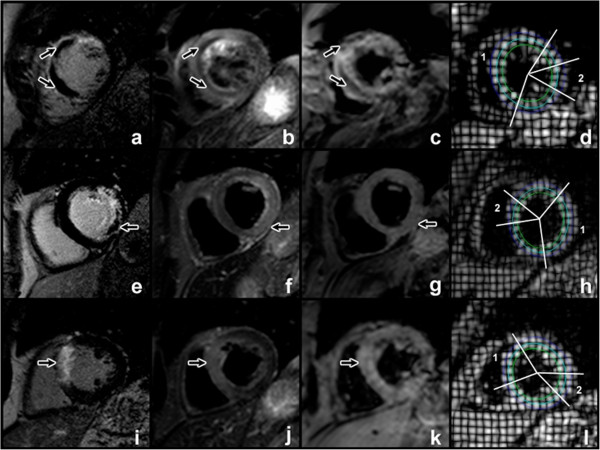
Methods: Thirty-nine patients underwent cardiovascular magnetic resonance (CMR) with T2-weighted and T2* imaging, late gadolinium enhancement (LGE) and myocardial tagging at 2, 7, 30 and 90 days following primary percutaneous coronary intervention for AMI. Circumferential strain in infarct and remote zones was stratified by presence of MO and IMH.
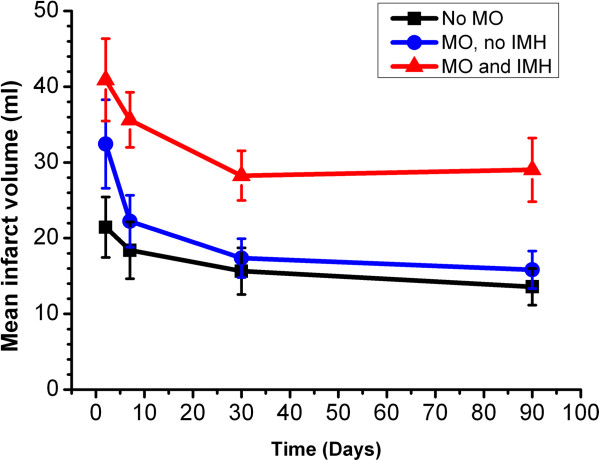
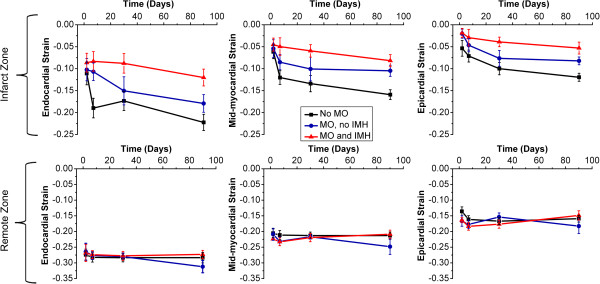
Results: Overall, infarct zone strain recovered with time (p < 0.001). In the presence of MO with IMH and without IMH, epicardial strain recovered (p = 0.03, p < 0.01 respectively), but mid-myocardial or endocardial strain did not (mid-myocardium: p = 0.05, p = 0.12; endocardium: p = 0.27, p = 0.05, respectively). By day 90, infarcts with MO had more attenuated strain in all myocardial layers compared to infarcts without MO (p < 0.01); those with IMH were attenuated further (p < 0.01). Remote myocardial strain was similar across groups at all time-points (p > 0.2). Infarct transmural extent did not correlate with strain (p > 0.05 at each time point). In multivariable logistic regression, MO and IMH were the only significant independent predictors of attenuated 90-day infarct zone strain (p = 0.004, p = 0.011, respectively).
Conclusions: Strain improves within the infarct zone overall following reperfusion with or without MO or IMH. Mid-myocardial and endocardial infarct contractility is diminished in the presence of MO, and further in the presence of IMH. MO and IMH are greater independent predictors of infarct zone contractile recovery than infarct volume or transmural extent.
Figures
References
-
- Morishima I, Sone T, Okumura K, Tsuboi H, Kondo J, Mukawa H, Matsui H, Toki Y, Ito T, Hayakawa T. Angiographic no-reflow phenomenon as a predictor of adverse long-term outcome in patients treated with percutaneous transluminal coronary angioplasty for first acute myocardial infarction. J Am Coll Cardiol. 2000;36:1202–9. doi: 10.1016/S0735-1097(00)00865-2. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
