

Frequency of EGFR and KRAS mutations in patients with non small cell lung cancer by racial background: do disparities exist?
- PMID: 23806795
- PMCID: PMC3749295
- DOI: 10.1016/j.lungcan.2013.05.011
Frequency of EGFR and KRAS mutations in patients with non small cell lung cancer by racial background: do disparities exist?
Abstract
Introduction: Mutations in EGFR and KRAS can impact treatment decisions for patients with NSCLC. The incidence of these mutations varies, and it is unclear whether there is a decreased frequency among African Americans (AfAs).
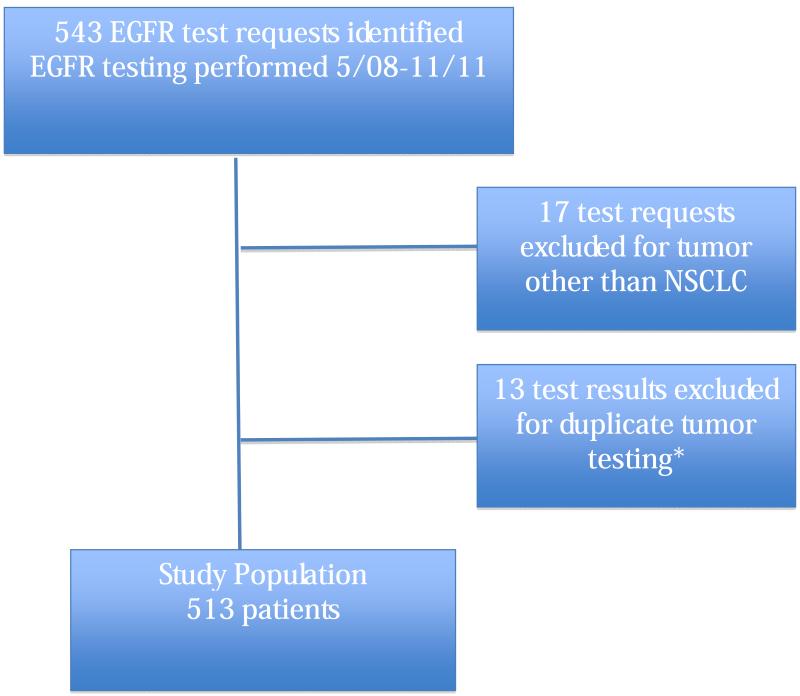
Methods: We performed a retrospective chart review of 513 NSCLC patients undergoing EGFR and KRAS mutational analysis at the Hospital of the University of Pennsylvania between May 2008 and November 2011. Clinical and pathologic data were abstracted from the patients' electronic medical record.
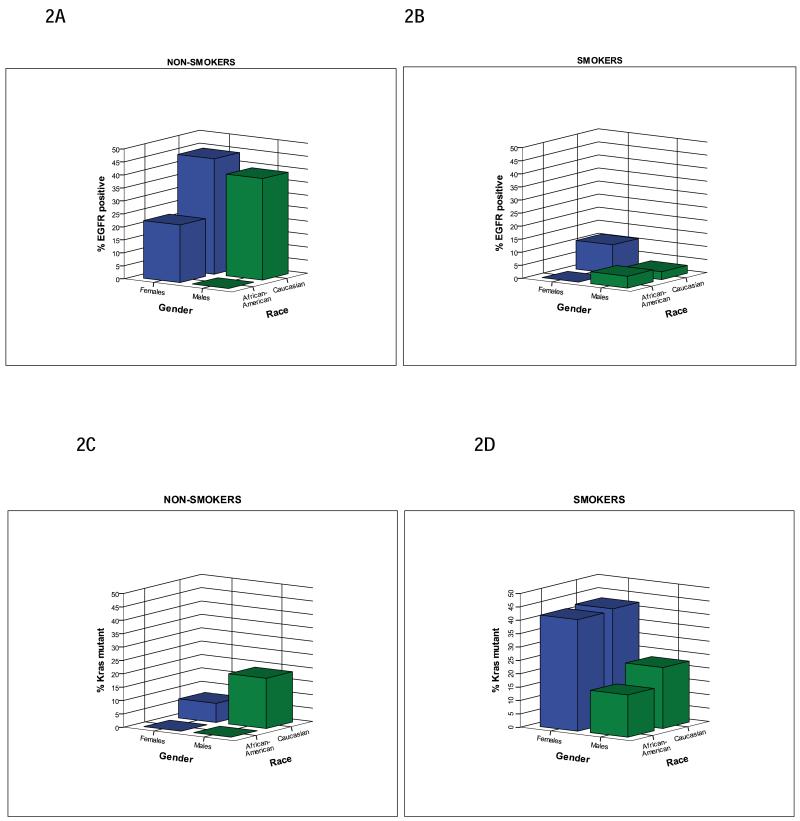
Results: Of 497 patients with informative EGFR mutation analyses, the frequency of EGFR mutation was 13.9%. The frequency of EGFR mutations was associated with race (p < 0.001) and was lower in AfA patients compared to Caucasian (C) patients but did not reach statistical significance (4.8% vs. 13.7%, p = 0.06). Mean Charlson Comorbidity Index and number of cigarette pack years were significantly lower in patients with EGFR mutations (p = 0.01 and p < 0.001, respectively). Multivariable logistic regression analysis showed a significant association between race and EGFR mutation (p = 0.01), even after adjusting for smoking status (p < 0.001) and gender (p = 0.03). KRAS mutation (study frequency 28.1%) was not associated with race (p = 0.08; p=0.51 for Afa vs. C patients), but was more common among smokers (p < 0.001) and females (p = 0.01).
Conclusions: Based on multivariable analysis, even after adjusting for smoking status and gender, we found that race was statistically significantly associated with EGFR mutation, but not KRAS mutational status. To the best of our knowledge, this is the largest single institution series to date evaluating racial differences in EGFR and KRAS mutational status among patients with NSCLC.
Keywords: EGFR; KRAS; NSCLC; Racial disparity.
Copyright © 2013 Elsevier Ireland Ltd. All rights reserved.
Figures
References
-
- Siegel R, Naishadham D, Jemal A. Cancer statistics, 2012. CA: a cancer journal for clinicians. 2012;62(1):10–29. doi: papers2://publication/doi/10.3322/caac.20138. - PubMed
-
- Zhou C, Wu Y-L, Chen G, Feng J, Liu X-Q, Wang C, et al. Erlotinib versus chemotherapy as first-line treatment for patients with advanced EGFR mutation-positive non-small-cell lung cancer (OPTIMAL, CTONG-0802): a multicentre, open-label, randomised, phase 3 study. The lancet oncology. 2011;12(8):735–42. doi: papers2://publication/doi/10.1016/S1470-2045(11)70184-X. - PubMed
-
- Fukuoka M, Wu Y-L, Thongprasert S, Sunpaweravong P, Leong S-S, Sriuranpong V, et al. Biomarker analyses and final overall survival results from a phase III, randomized, open-label, first-line study of gefitinib versus carboplatin/paclitaxel in clinically selected patients with advanced non-small-cell lung cancer in Asia (IPASS) Journal of clinical oncology: official journal of the American Society of Clinical Oncology. 2011;29(21):2866–74. doi: papers2://publication/doi/10.1200/JCO.2010.33.4235. - PubMed
-
- Lynch TJ, Bell DW, Sordella R, Gurubhagavatula S, Okimoto RA, Brannigan BW, et al. Activating mutations in the epidermal growth factor receptor underlying responsiveness of non-small-cell lung cancer to gefitinib. The New England journal of medicine. 2004;350(21):2129–39. doi: papers2://publication/doi/10.1056/NEJMoa040938. - PubMed
-
- Lee JS, Park K, Kim SW. A randomized phase III study of gefitinib versus standard chemotherapy (gemcitabine plus cisplatin) as a first-line treatment fornever-smokers with advanced or metastatic adenocarcinoma of the lung; World Conference on Lung Cancer; 2009; doi: papers2://publication/uuid/6B768E63-9B38-45C6-BEA3-C3BCB9556889.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
