

Using administrative data to identify naturally occurring networks of physicians
- PMID: 23807593
- PMCID: PMC3723338
- DOI: 10.1097/MLR.0b013e3182977991
Using administrative data to identify naturally occurring networks of physicians
Abstract
Background: Physicians naturally form networks. Networks could form a rational basis for Accountable Care Organizations (ACOs) for defined populations of Medicare beneficiaries.
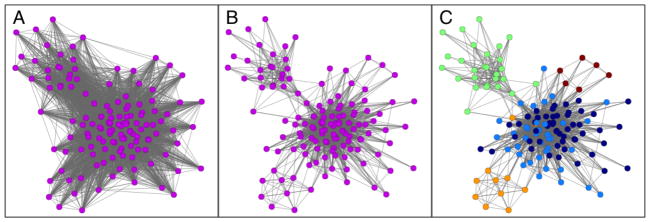
Objectives: To use methods from network science to identify naturally occurring networks of physicians that might be best suited to becoming ACOs.
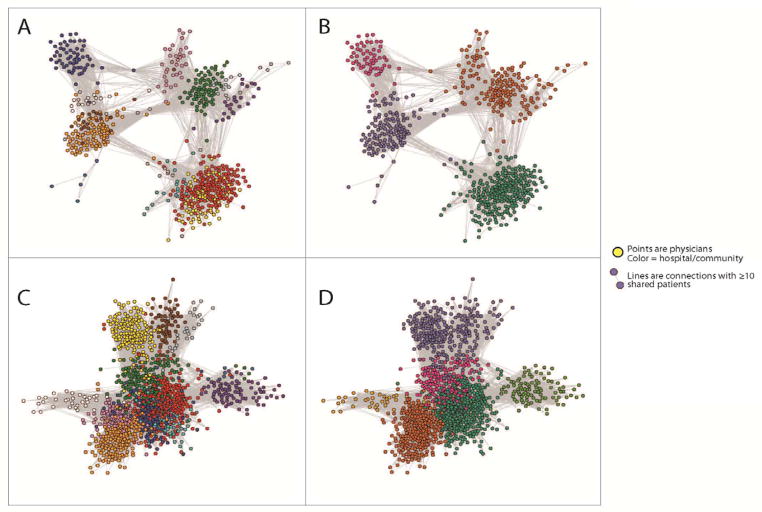
Research design, subjects, and measures: Using nationally representative claims data from the Medicare program for CY 2006 on 51 hospital referral regions (HRRs), we used a network science-based community-detection algorithm to identify groups of physicians likely to have preestablished relationships. After assigning patients to networks based upon visits with a primary care physician, we examined the proportion of care delivered within communities and compared our results with potential ACOs organized around single hospitals.
Results: We studied 4,586,044 Medicare beneficiaries from 51 HRRs who were seen by 68,288 active physicians practicing in those HRRs. The median community-based network ACO had 150 physicians with 5928 ties, whereas the median hospital-based network ACO had 96 physicians with 3276 ties. Among patients assigned to networks via their primary care physicians, seventy-seven percent of physician visits occurred with physicians in the community-based networks as compared with 56% with physicians in the hospital-based networks; however, just 8% of specialist visits were to specialists within the hospital-based networks as compared with 60% of specialist visits within the community-based networks. Some markets seemed better suited to developing ACOs based on network communities than others.
Conclusions: We present a novel approach to identifying groups of physicians that might readily function as ACOs. Organic networks identified and defined in this natural and systematic manner already have physicians who exhibit close working relationships, and who, importantly, keep the vast majority of care within the networks.
Figures
Similar articles
-
Variation in patient-sharing networks of physicians across the United States.JAMA. 2012 Jul 18;308(3):265-73. doi: 10.1001/jama.2012.7615. JAMA. 2012. PMID: 22797644 Free PMC article.
-
Patient-Sharing Networks of Physicians and Health Care Utilization and Spending Among Medicare Beneficiaries.JAMA Intern Med. 2018 Jan 1;178(1):66-73. doi: 10.1001/jamainternmed.2017.5034. JAMA Intern Med. 2018. PMID: 29181504 Free PMC article.
-
Multispecialty physician networks in Ontario.Open Med. 2013 May 14;7(2):e40-55. eCollection 2013. Open Med. 2013. PMID: 24348884 Free PMC article.
-
Outpatient care patterns and organizational accountability in Medicare.JAMA Intern Med. 2014 Jun;174(6):938-45. doi: 10.1001/jamainternmed.2014.1073. JAMA Intern Med. 2014. PMID: 24756690
-
Distribution of Visits for Chronic Conditions Between Primary Care and Specialist Providers in Medicare Shared Savings Accountable Care Organizations.Med Care. 2018 May;56(5):424-429. doi: 10.1097/MLR.0000000000000903. Med Care. 2018. PMID: 29634633
Cited by
-
Transitions of care across hospital settings in patients with inflammatory bowel disease.World J Gastroenterol. 2019 May 7;25(17):2122-2132. doi: 10.3748/wjg.v25.i17.2122. World J Gastroenterol. 2019. PMID: 31114138 Free PMC article.
-
Longitudinal Trends in Insurer Participation in Multisector Population Health Activities.Inquiry. 2024 Jan-Dec;61:469580241249092. doi: 10.1177/00469580241249092. Inquiry. 2024. PMID: 38742676 Free PMC article.
-
Representation of the hierarchical and functional structure of an ambulatory network of medical consultations through Social Network Analysis, with an emphasis on the role of medical specialties.PLoS One. 2024 Feb 15;19(2):e0290596. doi: 10.1371/journal.pone.0290596. eCollection 2024. PLoS One. 2024. PMID: 38359023 Free PMC article.
-
Quantification of the resilience of primary care networks by stress testing the health care system.Proc Natl Acad Sci U S A. 2019 Nov 26;116(48):23930-23935. doi: 10.1073/pnas.1904826116. Epub 2019 Nov 11. Proc Natl Acad Sci U S A. 2019. PMID: 31712415 Free PMC article.
-
Provider Connectedness to Other Providers Reduces Risk of Readmission After Hospitalization for Heart Failure.Med Care Res Rev. 2019 Feb;76(1):115-128. doi: 10.1177/1077558717718626. Epub 2017 Jul 8. Med Care Res Rev. 2019. PMID: 29148301 Free PMC article.
References
-
- Fortunato S. Community detection in graphs. Physics Reports. 2010;486:75–174.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
