

Osteoporosis - a current view of pharmacological prevention and treatment
- PMID: 23807838
- PMCID: PMC3686324
- DOI: 10.2147/DDDT.S31504
Osteoporosis - a current view of pharmacological prevention and treatment
Abstract
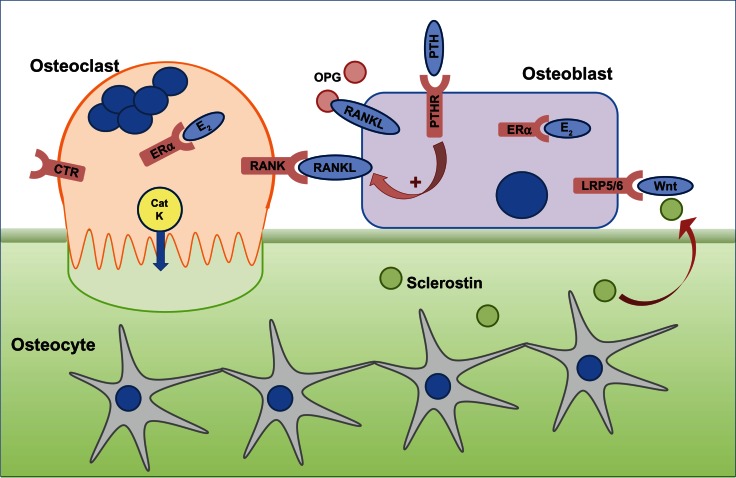
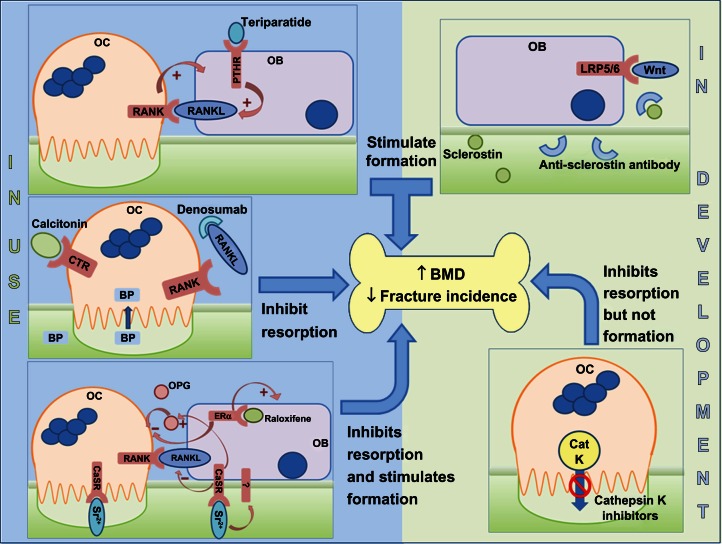
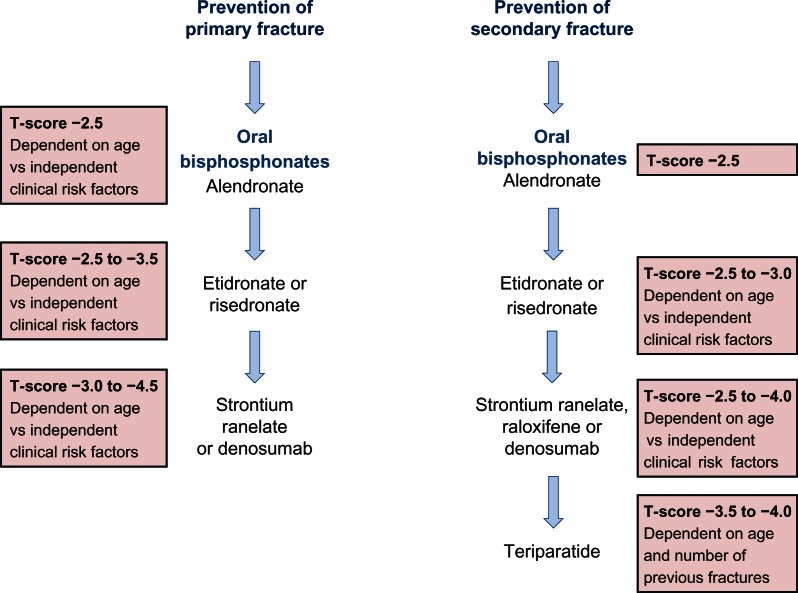
Postmenopausal osteoporosis is the most common bone disease, associated with low bone mineral density (BMD) and pathological fractures which lead to significant morbidity. It is defined clinically by a BMD of 2.5 standard deviations or more below the young female adult mean (T-score =-2.5). Osteoporosis was a huge global problem both socially and economically - in the UK alone, in 2011 £6 million per day was spent on treatment and social care of the 230,000 osteoporotic fracture patients - and therefore viable preventative and therapeutic approaches are key to managing this problem within the aging population of today. One of the main issues surrounding the potential of osteoporosis management is diagnosing patients at risk before they develop a fracture. We discuss the current and future possibilities for identifying susceptible patients, from fracture risk assessment to shape modeling and in relation to the high heritability of osteoporosis now that a plethora of genes have been associated with low BMD and osteoporotic fracture. This review highlights the current therapeutics in clinical use (including bisphosphonates, anti-RANKL [receptor activator of NF-κB ligand], intermittent low dose parathyroid hormone, and strontium ranelate) and some of those in development (anti-sclerostin antibodies and cathepsin K inhibitors). By highlighting the intimate relationship between the activities of bone forming (osteoblasts) and bone-resorbing (osteoclasts) cells, we include an overview and comparison of the molecular mechanisms exploited in each therapy.
Keywords: BMD; bisphosphonate; denosumab; fracture; raloxifene; strontium; teriparatide.
Figures

Similar articles
-
Treatment of post-menopausal osteoporosis: beyond bisphosphonates.J Endocrinol Invest. 2015 Jan;38(1):13-29. doi: 10.1007/s40618-014-0152-z. Epub 2014 Sep 7. J Endocrinol Invest. 2015. PMID: 25194424 Review.
-
Osteoporosis: now and the future.Lancet. 2011 Apr 9;377(9773):1276-87. doi: 10.1016/S0140-6736(10)62349-5. Epub 2011 Mar 28. Lancet. 2011. PMID: 21450337 Free PMC article. Review.
-
Denosumab, raloxifene, romosozumab and teriparatide to prevent osteoporotic fragility fractures: a systematic review and economic evaluation.Health Technol Assess. 2020 Jun;24(29):1-314. doi: 10.3310/hta24290. Health Technol Assess. 2020. PMID: 32588816 Free PMC article.
-
The cost effectiveness of bisphosphonates for the prevention and treatment of osteoporosis: a structured review of the literature.Pharmacoeconomics. 2007;25(11):913-33. doi: 10.2165/00019053-200725110-00003. Pharmacoeconomics. 2007. PMID: 17960951 Review.
-
Antifracture efficacy of currently available therapies for postmenopausal osteoporosis.Drugs. 2011 Jan 1;71(1):65-78. doi: 10.2165/11587570-000000000-00000. Drugs. 2011. PMID: 21175240 Review.
Cited by
-
Nano-Based Biomaterials as Drug Delivery Systems Against Osteoporosis: A Systematic Review of Preclinical and Clinical Evidence.Nanomaterials (Basel). 2021 Feb 19;11(2):530. doi: 10.3390/nano11020530. Nanomaterials (Basel). 2021. PMID: 33669621 Free PMC article. Review.
-
The Role and Mechanism of SIRT1 in Resveratrol-regulated Osteoblast Autophagy in Osteoporosis Rats.Sci Rep. 2019 Dec 5;9(1):18424. doi: 10.1038/s41598-019-44766-3. Sci Rep. 2019. PMID: 31804494 Free PMC article.
-
The effect of Lycii Radicis Cortex extract on bone formation in vitro and in vivo.Molecules. 2014 Nov 26;19(12):19594-609. doi: 10.3390/molecules191219594. Molecules. 2014. PMID: 25432011 Free PMC article.
-
Sclerostin antibody prevented progressive bone loss in combined ovariectomized and concurrent functional disuse.Bone. 2016 Jun;87:161-8. doi: 10.1016/j.bone.2016.02.005. Epub 2016 Feb 8. Bone. 2016. PMID: 26868528 Free PMC article.
-
Effects of minodronate in postmenopausal women with osteoporosis who received prior treatment with raloxifene.Int J Womens Health. 2017 Nov 13;9:821-825. doi: 10.2147/IJWH.S145805. eCollection 2017. Int J Womens Health. 2017. PMID: 29180905 Free PMC article.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
