

Leukoreduction and ultraviolet treatment reduce both the magnitude and the duration of the HLA antibody response
- PMID: 23808544
- PMCID: PMC3825847
- DOI: 10.1111/trf.12317
Leukoreduction and ultraviolet treatment reduce both the magnitude and the duration of the HLA antibody response
Abstract
Background: Both leukoreduction and ultraviolet (UV) light treatment of blood products have been shown to reduce the incidence of HLA antibody development in recipients, but the impact of these treatments on the magnitude and persistence of the antibody response is less clear.
Study design and methods: Longitudinal samples from 319 subjects taken from four different study cohorts were evaluated for HLA antibodies to determine the effects of leukoreduction and UV treatment on HLA antibody generation and persistence.
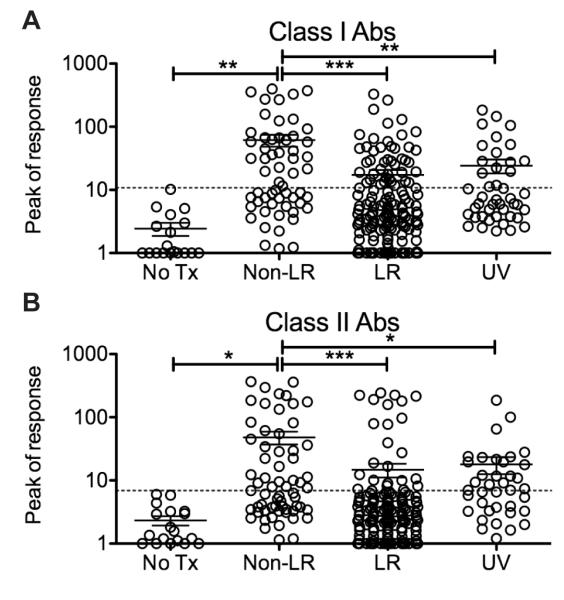
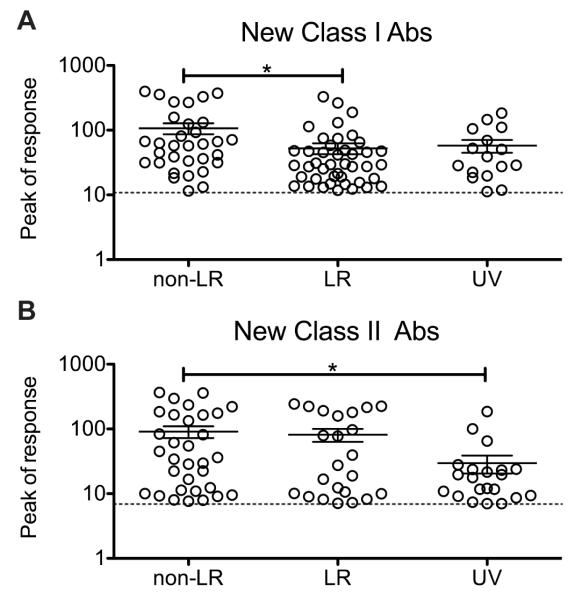
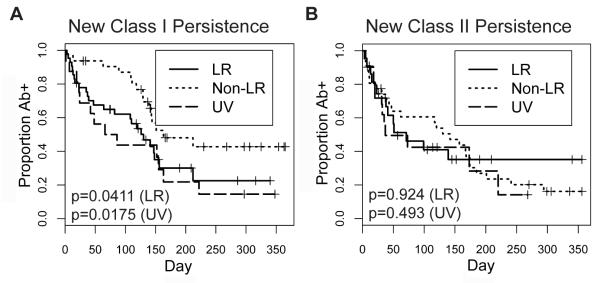
Results: Subjects receiving leukoreduced or UV-treated blood products were less likely to generate Class I HLA antibodies, and those receiving leukoreduced blood were also less likely to generate Class II HLA antibodies. Among those receiving nonleukoreduced blood, 55% developed Class I HLA antibodies and 51% developed Class II HLA antibodies compared with 28% (Class I) and 15% (Class II) for those receiving leukoreduced blood and 36% (Class I) and 54% (Class II) for those receiving UV-treated blood. Among alloimmunized subjects, leukoreduction resulted in a significant twofold reduction in the magnitude of Class I HLA antibodies, and UV treatment resulted in a significant threefold reduction in the magnitude of Class II HLA antibodies. Both treatments resulted in shorter persistence of Class I HLA antibodies.
Conclusions: These data demonstrate that leukoreduction and UV treatment of blood products results not only in a reduction in the incidence of HLA antibody production, but also in lower and more transient HLA antibody levels among sensitized transfusion recipients.
© 2013 American Association of Blood Banks.
Figures
References
-
- Cox JV, Steane E, Cunningham G, Frenkel EP. Risk of alloimmunization and delayed hemolytic transfusion reactions in patients with sickle cell disease. Archives of Internal Medicine. 1988;148:2485–9. - PubMed
-
- Michail-Merianou V, Pamphili-Panousopoulou L, Piperi-Lowes L, Pelegrinis E, Karaklis A. Alloimmunization to red cell antigens in thalassemia: comparative study of usual versus better-match transfusion programmes. Vox Sang. 1987;52:95–8. - PubMed
-
- Orlina AR, Unger PJ, Koshy M. Post-transfusion alloimmunization in patients with sickle cell disease. Am J Hematol. 1978;5:101–6. - PubMed
-
- Rosse WF, Gallagher D, Kinney TR, Castro O, Dosik H, Moohr J, Wang W, Levy PS. Transfusion and alloimmunization in sickle cell disease. The Cooperative Study of Sickle Cell Disease. Blood. 1990;76:1431–7. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
