

Accountable care organizations: benefits and barriers as perceived by Rural Health Clinic management
- PMID: 23808801
- PMCID: PMC3761377
Accountable care organizations: benefits and barriers as perceived by Rural Health Clinic management
Abstract
Introduction: Rural Health Clinics (RHCs) have served the primary healthcare needs of the medically underserved in US rural areas for more than 30 years. As a new model of healthcare delivery, the Accountable Care Organization (ACO) offers potential opportunities for addressing the healthcare needs of rural populations, yet little is known about how the ACO model will meet the needs of RHCs. This article reports on the results of a survey, focus groups, and phone interviews with RHC management personnel on the subject of benefits of and barriers to RHC participation in ACOs.
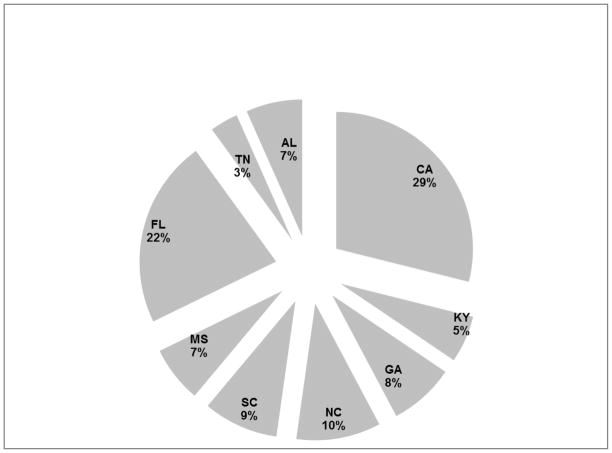
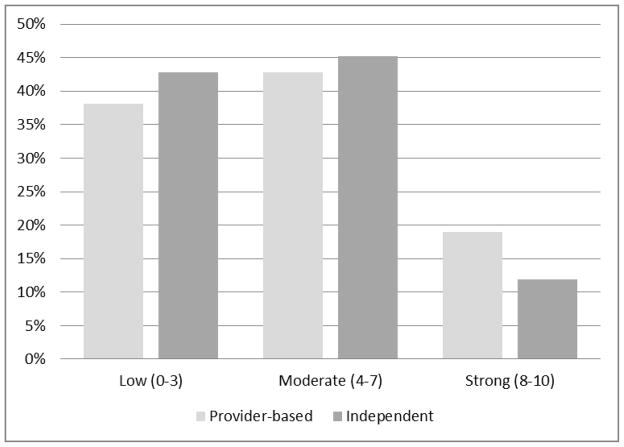
Methods: Survey research, focus groups, and phone interviews were used to gather and analyze the opinions of RHCs' management about the benefits of and barriers to ACO participation. The study population consisted of all 2011 RHCs in Region 4 (Southeastern USA; as designated by the Department of Health and Human Services). California RHCs were used for comparison. Themes and concepts for the survey questionnaire were developed from recent literature. The survey data were analyzed in two stages: (1) analyses of the characteristics of the RHCs and their responses; and (2) bivariate analyses of several relationships using a variety of statistics including analysis of variance, Pearson's χ² and likelihood χ². Relationships were examined between the RHCs' willingness to join ACOs and the respondent clinic's classification (as provider-based or independent). In addition, willingness to join ACOs among Region 4 RHCs was compared with those in California. Finally, in order to gain a broader understanding of the results of the survey, focus groups and phone interviews were conducted with RHC personnel.
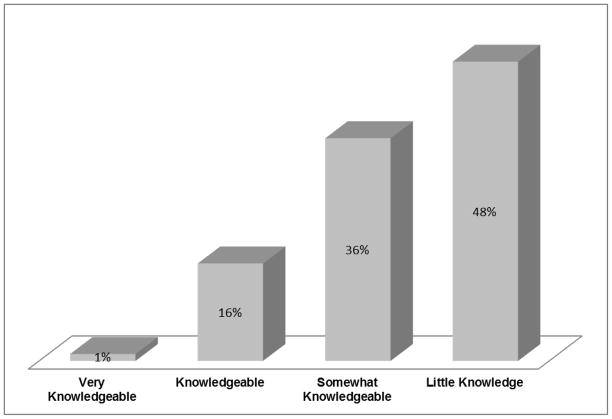
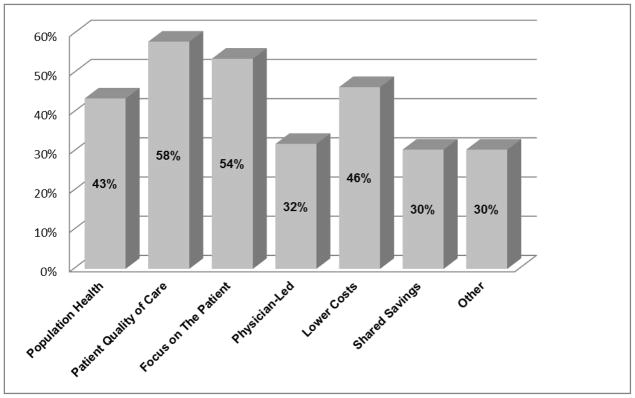
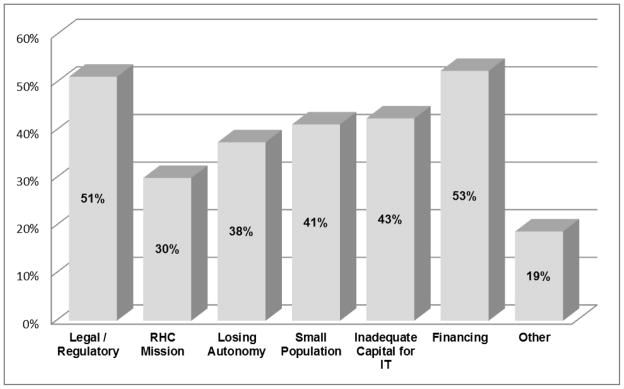
Results: It was found that the ACO model is generally unfamiliar to RHCs. Approximately 48% of the survey respondents reported having little knowledge of ACOs; the focus group participants and interviewees likewise reported a lack of knowledge. Among respondents who were knowledgeable about ACOs, the most frequently citied potential benefit of ACOs (58%) was improved patient quality of care, followed by a focus on the patient (54%). More than half of the respondents (53%) cited 'financing' as a deterrent to RHC participating in ACOs. Many (43%) reported that their clinic had inadequate capital to improve their information technology systems. Another 51% cited legal and regulatory barriers.
Conclusions: While the ACO model was unfamiliar to many of the RHC study participants, many suggested that ACOs may promote the quality of health care for RHC patients and their communities. If, on the other hand, RHCs are not provided the necessary technical assistance or not valued as ACO partners, ACOs may not improve the services that RHCs provide. As the ACO model evolves, the authors will determine whether it will benefit RHCs and their patients, or how the ACO must be modified to accommodate the unique needs of RHCs.
Figures
References
-
- MacKinney AC, Mueller KJ, McBride TD. The march to Accountable Care Organizations-How will rural fare? Journal of rural health. 2011;27(1):131–137. - PubMed
-
- Croshaw A. [Accessed 17 July 2012];Growth and dispersion of Accountable Care Organizations. Available: http://leavittpartnersblog.com/2011/11.
-
- Shortell SM, Casalino LP, Fisher ES. How the Center for Medicare and Medicaid innovation should test accountable care organizations. Health Affairs. 2010;29 (7):1293–1298. - PubMed
-
- Shields MC, Patel PH, Manning M, Sacks L. A model for integrating independent physicians into Accountable Care Organizations. Health Affairs. 2011;30(1):161–172. - PubMed
-
- Shortell SM, Casalino LP. Implementing qualifications criteria and technical assistance for Accountable Care Organizations. JAMA-Journal of the American Medical Association. 2010;303(17):1747–1748. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
