

Chest radiography for predicting the cause of febrile illness among inpatients in Moshi, Tanzania
- PMID: 23809268
- PMCID: PMC3759645
- DOI: 10.1016/j.crad.2013.05.002
Chest radiography for predicting the cause of febrile illness among inpatients in Moshi, Tanzania
Abstract
Aim: To describe chest radiographic abnormalities and assess their usefulness for predicting causes of fever in a resource-limited setting.
Materials and methods: Febrile patients were enrolled in Moshi, Tanzania, and chest radiographs were evaluated by radiologists in Tanzania and the United States. Radiologists were blinded to the results of extensive laboratory evaluations to determine the cause of fever.
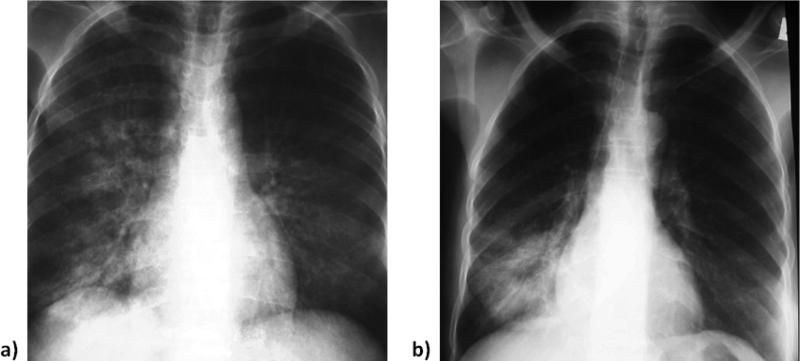
Results: Of 870 febrile patients, 515 (59.2%) had a chest radiograph available; including 268 (66.5%) of the adolescents and adults, the remainder were infants and children. One hundred and nineteen (44.4%) adults and 51 (20.6%) children were human immunodeficiency virus (HIV)-infected. Among adults, radiographic abnormalities were present in 139 (51.9%), including 77 (28.7%) with homogeneous and heterogeneous lung opacities, 26 (9.7%) with lung nodules, 25 (9.3%) with pleural effusion, 23 (8.6%) with cardiomegaly, and 13 (4.9%) with lymphadenopathy. Among children, radiographic abnormalities were present in 87 (35.2%), including 76 (30.8%) with homogeneous and heterogeneous lung opacities and six (2.4%) with lymphadenopathy. Among adolescents and adults, the presence of opacities was predictive of Streptococcus pneumoniae and Coxiella burnetii, whereas the presence of pulmonary nodules was predictive of Histoplasma capsulatum and Cryptococcus neoformans.
Conclusions: Chest radiograph abnormalities among febrile inpatients are common in northern Tanzania. Chest radiography is a useful adjunct for establishing an aetiologic diagnosis of febrile illness and may provide useful information for patient management, in particular for pneumococcal disease, Q fever, and fungal infections.
Copyright © 2013 The Royal College of Radiologists. Published by Elsevier Ltd. All rights reserved.
Figures

Similar articles
-
Q fever, spotted fever group, and typhus group rickettsioses among hospitalized febrile patients in northern Tanzania.Clin Infect Dis. 2011 Aug;53(4):e8-15. doi: 10.1093/cid/cir411. Clin Infect Dis. 2011. PMID: 21810740 Free PMC article.
-
Leptospirosis and human immunodeficiency virus co-infection among febrile inpatients in northern Tanzania.Vector Borne Zoonotic Dis. 2013 Aug;13(8):572-80. doi: 10.1089/vbz.2012.1205. Epub 2013 May 10. Vector Borne Zoonotic Dis. 2013. PMID: 23663165 Free PMC article.
-
Invasive bacterial and fungal infections among hospitalized HIV-infected and HIV-uninfected children and infants in northern Tanzania.Trop Med Int Health. 2011 Jul;16(7):830-7. doi: 10.1111/j.1365-3156.2011.02774.x. Epub 2011 Apr 7. Trop Med Int Health. 2011. PMID: 21470347 Free PMC article.
-
Chest radiographic pulmonary changes reflecting extrapulmonary involvement in paediatric HIV disease.Pediatr Radiol. 2009 Jun;39(6):565-8. doi: 10.1007/s00247-009-1162-4. Epub 2009 Feb 24. Pediatr Radiol. 2009. PMID: 19238372 Review.
-
Interpretation of chest radiographs in infants with cough and fever.Radiology. 2005 Jul;236(1):22-9. doi: 10.1148/radiol.2361041278. Epub 2005 Jun 27. Radiology. 2005. PMID: 15983074 Review.
Cited by
-
Epidemiology of Coxiella burnetii infection in Africa: a OneHealth systematic review.PLoS Negl Trop Dis. 2014 Apr 10;8(4):e2787. doi: 10.1371/journal.pntd.0002787. eCollection 2014 Apr. PLoS Negl Trop Dis. 2014. PMID: 24722554 Free PMC article.
References
-
- Petit PL, van Ginneken JK. Analysis of hospital records in four African countries, 1975–1990, with emphasis on infectious diseases. J Trop Med Hyg. 1995;98:217–27. - PubMed
-
- Bahwere P, Levy J, Hennart P, et al. Community-acquired bacteremia among hospitalized children in rural central Africa. Int J Infect Dis. 2001;5:180–8. - PubMed
-
- Peters RP, Zijlstra EE, Schijffelen MJ, et al. A prospective study of bloodstream infections as cause of fever in Malawi: clinical predictors and implications for management. Trop Med Int Health. 2004;9:928–34. - PubMed
-
- Parker TM, Murray CK, Richards AL, et al. Concurrent infections in acute febrile illness patients in Egypt. Am J Trop Med Hyg. 2007;77:390–2. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
