

Decentralized cardiovascular autonomic control and cognitive deficits in persons with spinal cord injury
- PMID: 23809520
- PMCID: PMC3595971
- DOI: 10.1179/2045772312Y.0000000056
Decentralized cardiovascular autonomic control and cognitive deficits in persons with spinal cord injury
Abstract
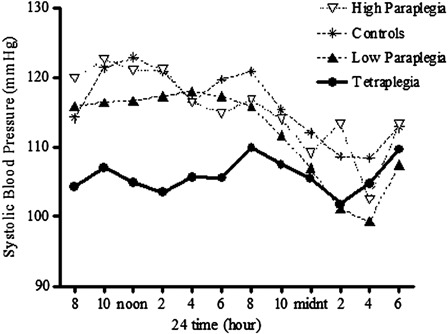
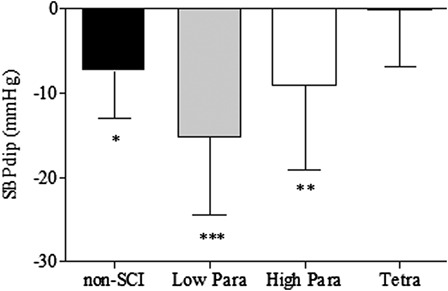
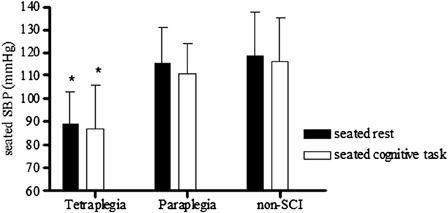
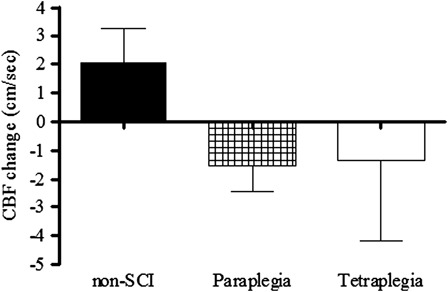
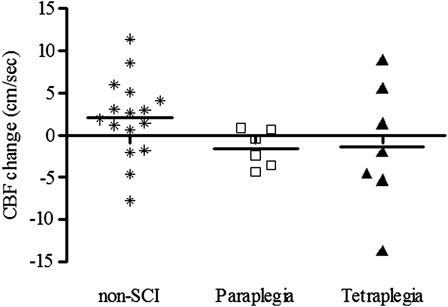
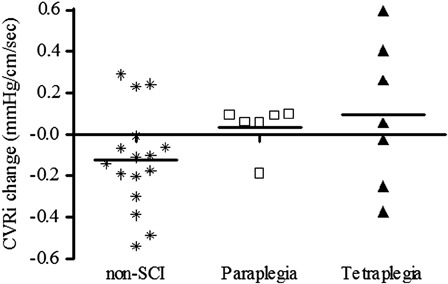
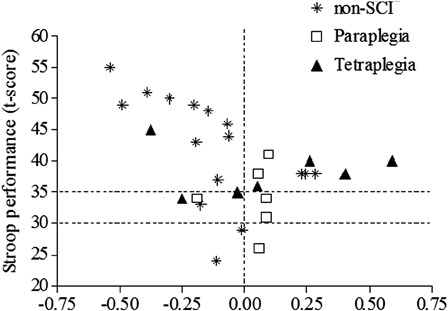
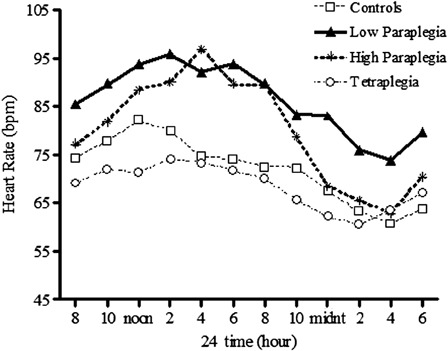
Spinal cord injury (SCI) results in motor and sensory impairments that can be identified with the American Spinal Injury Association (ASIA) Impairment Scale (AIS). Although, SCI may disrupt autonomic neural transmission, less is understood regarding the clinical impact of decentralized autonomic control. Cardiovascular regulation may be altered following SCI and the degree of impairment may or may not relate to the level of AIS injury classification. In general, persons with lesions above T1 present with bradycardia, hypotension, and orthostatic hypotension; functional changes which may interfere with rehabilitation efforts. Although many individuals with SCI above T1 remain overtly asymptomatic to hypotension, we have documented deficits in memory and attention processing speed in hypotensive individuals with SCI compared to a normotensive SCI cohort. Reduced resting cerebral blood flow (CBF) and diminished CBF responses to cognitive testing relate to test performance in hypotensive non-SCI, and preliminary evidence suggests a similar association in individuals with SCI. Persons with paraplegia below T7 generally present with a normal cardiovascular profile; however, our group and others have documented persistently elevated heart rate and increased arterial stiffness. In the non-SCI literature there is evidence supporting a link between increased arterial stiffness and cognitive deficits. Preliminary evidence suggests increased incidence of cognitive impairment in individuals with paraplegia, which we believe may relate to adverse cardiovascular changes. This report reviews relevant literature and discusses findings related to the possible association between decentralized cardiovascular autonomic control and cognitive dysfunction in persons with SCI.
Figures
References
-
- Davidoff G, Morris J, Roth E, Bleiberg J. Cognitive dysfunction and mild closed head injury in traumatic spinal cord injury. Arch Phys Med Rehabil 1985;66(8):489–91 - PubMed
-
- Davidoff G, Roth E, Thomas P, Doljanac R, Dijkers M, Berent S, et al. Depression and neuropsychological test performance in acute spinal cord injury patients: lack of correlation. Arch Clin Neuropsychol 1990;5(1):77–88 - PubMed
-
- Davidoff GN, Roth EJ, Haughton JS, Ardner MS. Cognitive dysfunction in spinal cord injury patients: sensitivity of the Functional Independence Measure subscales vs neuropsychologic assessment. Arch Phys Med Rehabil 1990;71(5):326–9 - PubMed
-
- Roth E, Davidoff G, Thomas P, Doljanac R, Dijkers M, Berent S, et al. A controlled study of neuropsychological deficits in acute spinal cord injury patients. Paraplegia 1989;27(6):480–9 - PubMed
-
- Wilmot CB, Cope DN, Hall KM, Acker M. Occult head injury: its incidence in spinal cord injury. Arch Phys Med Rehabil 1985;66(4):227–31 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical