

Exserohilum infections associated with contaminated steroid injections: a clinicopathologic review of 40 cases
- PMID: 23809916
- PMCID: PMC4401815
- DOI: 10.1016/j.ajpath.2013.05.007
Exserohilum infections associated with contaminated steroid injections: a clinicopathologic review of 40 cases
Abstract
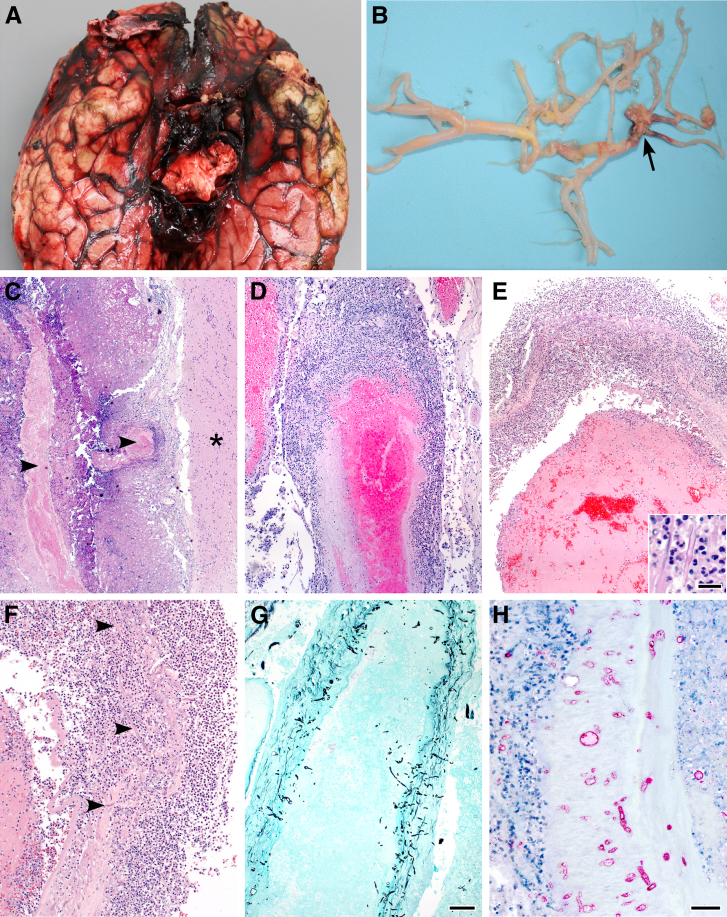
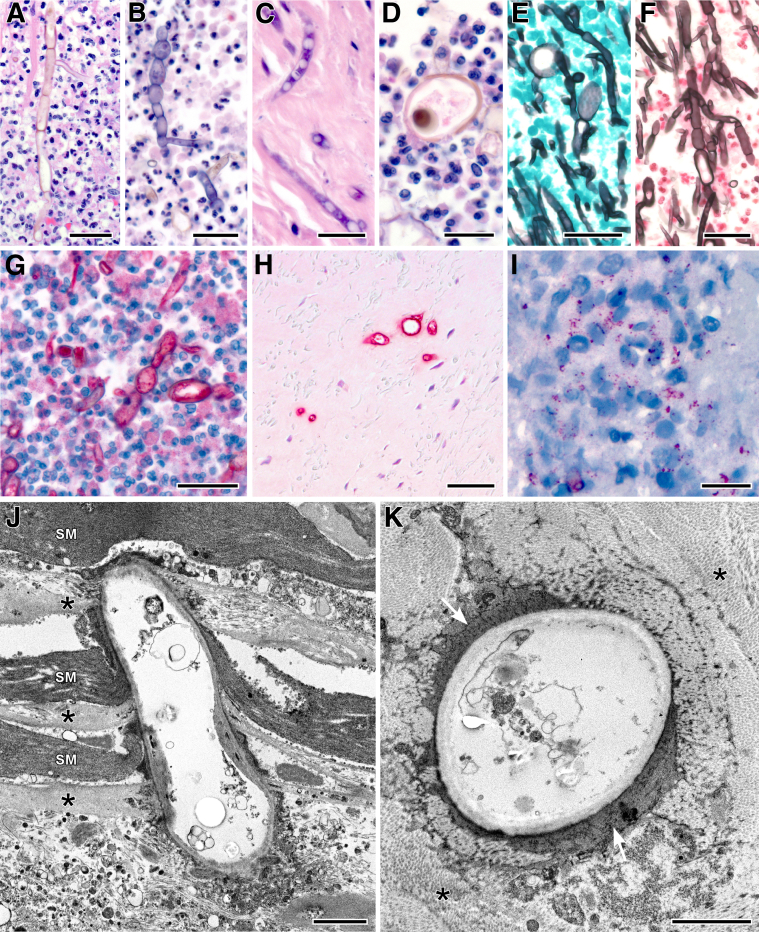
September 2012 marked the beginning of the largest reported outbreak of infections associated with epidural and intra-articular injections. Contamination of methylprednisolone acetate with the black mold, Exserohilum rostratum, was the primary cause of the outbreak, with >13,000 persons exposed to the potentially contaminated drug, 741 confirmed drug-related infections, and 55 deaths. Fatal meningitis and localized epidural, paraspinal, and peripheral joint infections occurred. Tissues from 40 laboratory-confirmed cases representing these various clinical entities were evaluated by histopathological analysis, special stains, and IHC to characterize the pathological features and investigate the pathogenesis of infection, and to evaluate methods for detection of Exserohilum in formalin-fixed, paraffin-embedded (FFPE) tissues. Fatal cases had necrosuppurative to granulomatous meningitis and vasculitis, with thrombi and abundant angioinvasive fungi, with extensive involvement of the basilar arterial circulation of the brain. IHC was a highly sensitive method for detection of fungus in FFPE tissues, demonstrating both hyphal forms and granular fungal antigens, and PCR identified Exserohilum in FFPE and fresh tissues. Our findings suggest a pathogenesis for meningitis involving fungal penetration into the cerebrospinal fluid at the injection site, with transport through cerebrospinal fluid to the basal cisterns and subsequent invasion of the basilar arteries. Further studies are needed to characterize Exserohilum and investigate the potential effects of underlying host factors and steroid administration on the pathogenesis of infection.
Copyright © 2013 American Society for Investigative Pathology. Published by Elsevier Inc. All rights reserved.
Figures

Comment in
-
Fungal disease following contaminated steroid injections: Exserohilum is ready for its close-up.Am J Pathol. 2013 Sep;183(3):661-4. doi: 10.1016/j.ajpath.2013.06.010. Epub 2013 Jul 19. Am J Pathol. 2013. PMID: 23876717 Free PMC article.
References
-
- Carrino J.A., Morrison W.B., Parker L., Schweitzer M.E., Levin D.C., Sunshine J.H. Spinal injection procedures: volume, provider distribution, and reimbursement in the U.S. medicare population from 1993 to 1999. Radiology. 2002;225:723–729. - PubMed
-
- Windsor R.E., Storm S., Sugar R. Prevention and management of complications resulting from common spinal injections. Pain Physician. 2003;6:473–483. - PubMed
-
- Derby R., Lee S.H., Kim B.J., Chen Y., Seo K.S. Complications following cervical epidural steroid injections by expert interventionalists in 2003. Pain Physician. 2004;7:445–449. - PubMed
-
- Kabbara A., Rosenberg S.K., Untal C. Methicillin-resistant Staphylococcus aureus epidural abscess after transforaminal epidural steroid injection. Pain Physician. 2004;7:269–272. - PubMed
-
- Gaul C., Neundörfer B., Winterholler M. Iatrogenic (para-) spinal abscesses and meningitis following injection therapy for low back pain. Pain. 2005;116:407–410. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
