

Genetic variation and HIV-associated neurologic disease
- PMID: 23809924
- PMCID: PMC4074542
- DOI: 10.1016/B978-0-12-407698-3.00006-5
Genetic variation and HIV-associated neurologic disease
Abstract
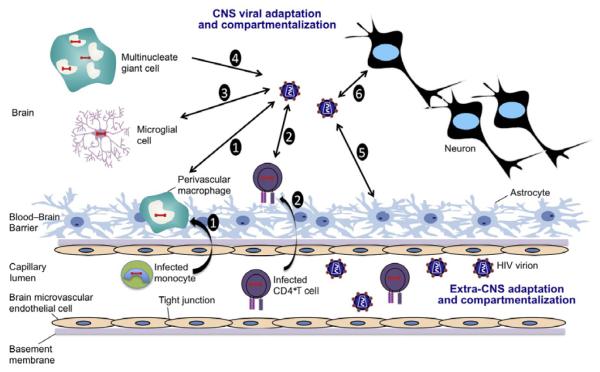
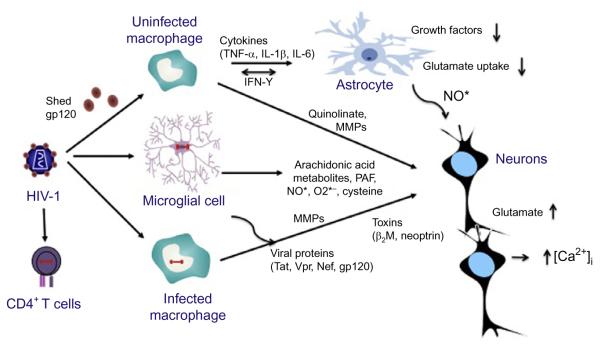
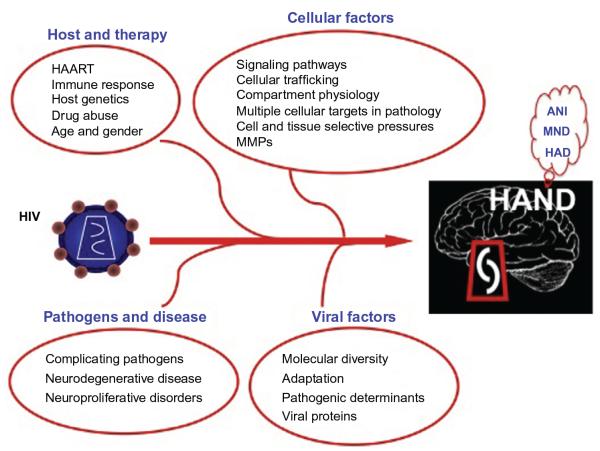
HIV-associated neurologic disease continues to be a significant complication in the era of highly active antiretroviral therapy. A substantial subset of the HIV-infected population shows impaired neuropsychological performance as a result of HIV-mediated neuroinflammation and eventual central nervous system (CNS) injury. CNS compartmentalization of HIV, coupled with the evolution of genetically isolated populations in the CNS, is responsible for poor prognosis in patients with AIDS, warranting further investigation and possible additions to the current therapeutic strategy. This chapter reviews key advances in the field of neuropathogenesis and studies that have highlighted how molecular diversity within the HIV genome may impact HIV-associated neurologic disease. We also discuss the possible functional implications of genetic variation within the viral promoter and possibly other regions of the viral genome, especially in the cells of monocyte-macrophage lineage, which are arguably key cellular players in HIV-associated CNS disease.
Copyright © 2013 Elsevier Inc. All rights reserved.
Figures
Similar articles
-
Development of co-selected single nucleotide polymorphisms in the viral promoter precedes the onset of human immunodeficiency virus type 1-associated neurocognitive impairment.J Neurovirol. 2011 Feb;17(1):92-109. doi: 10.1007/s13365-010-0014-1. Epub 2011 Jan 12. J Neurovirol. 2011. PMID: 21225391 Free PMC article.
-
Genetic and functional heterogeneity of CNS-derived tat alleles from patients with HIV-associated dementia.J Neurovirol. 2011 Feb;17(1):70-81. doi: 10.1007/s13365-010-0002-5. Epub 2010 Nov 30. J Neurovirol. 2011. PMID: 21165788
-
Compartmentalized human immunodeficiency virus type 1 originates from long-lived cells in some subjects with HIV-1-associated dementia.PLoS Pathog. 2009 Apr;5(4):e1000395. doi: 10.1371/journal.ppat.1000395. Epub 2009 Apr 24. PLoS Pathog. 2009. PMID: 19390619 Free PMC article.
-
Molecular pathway involved in HIV-1-induced CNS pathology: role of viral regulatory protein, Tat.J Leukoc Biol. 1999 Apr;65(4):458-65. doi: 10.1002/jlb.65.4.458. J Leukoc Biol. 1999. PMID: 10204574 Review.
-
HIV-Associated Neurotoxicity: The Interplay of Host and Viral Proteins.Mediators Inflamm. 2021 Aug 25;2021:1267041. doi: 10.1155/2021/1267041. eCollection 2021. Mediators Inflamm. 2021. PMID: 34483726 Free PMC article. Review.
Cited by
-
Human Immune System Mice for the Study of Human Immunodeficiency Virus-Type 1 Infection of the Central Nervous System.Front Immunol. 2018 Apr 4;9:649. doi: 10.3389/fimmu.2018.00649. eCollection 2018. Front Immunol. 2018. PMID: 29670623 Free PMC article. Review.
-
Interaction between Tat and Drugs of Abuse during HIV-1 Infection and Central Nervous System Disease.Front Microbiol. 2016 Jan 11;6:1512. doi: 10.3389/fmicb.2015.01512. eCollection 2015. Front Microbiol. 2016. PMID: 26793168 Free PMC article. Review.
-
Investigating the distribution of HIV-1 Tat lengths present in the Drexel Medicine CARES cohort.Virus Res. 2019 Oct 15;272:197727. doi: 10.1016/j.virusres.2019.197727. Epub 2019 Aug 19. Virus Res. 2019. PMID: 31437485 Free PMC article.
-
The Evolution of Dendritic Cell Immunotherapy against HIV-1 Infection: Improvements and Outlook.J Immunol Res. 2020 May 25;2020:9470102. doi: 10.1155/2020/9470102. eCollection 2020. J Immunol Res. 2020. PMID: 32537473 Free PMC article. Review.
-
Is human immunodeficiency virus-mediated dementia an autophagic defect that leads to neurodegeneration?CNS Neurol Disord Drug Targets. 2014;13(9):1571-9. doi: 10.2174/1871527313666140806125841. CNS Neurol Disord Drug Targets. 2014. PMID: 25106633 Free PMC article. Review.
References
-
- Addo MM, Yu XG, Rathod A, Cohen D, Eldridge RL, Strick D, et al. Comprehensive epitope analysis of human immunodeficiency virus type 1 (HIV-1)-specific T-cell responses directed against the entire expressed HIV-1 genome demonstrate broadly directed responses, but no correlation to viral load. Journal of Virology. 2003;77:2081. - PMC - PubMed
-
- Agrawal L, Maxwell CR, Peters PJ, Clapham PR, Liu SM, Mackay CR, et al. Complexity in human immunodeficiency virus type 1 (HIV-1) co-receptor usage: Roles of CCR3 and CCR5 in HIV-1 infection of monocyte-derived macrophages and brain microglia. The Journal of General Virology. 2009;90:710. - PubMed
-
- Alkhatib G, Combadiere C, Broder CC, Feng Y, Kennedy PE, Murphy PM, et al. CC CKR5: A RANTES, MIP-1alpha, MIP-1beta receptor as a fusion cofactor for macrophage-tropic HIV-1. Science. 1996;272:1955. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical