

Newborn screening for severe combined immunodeficiency and T-cell lymphopenia in California: results of the first 2 years
- PMID: 23810098
- PMCID: PMC3759317
- DOI: 10.1016/j.jaci.2013.04.024
Newborn screening for severe combined immunodeficiency and T-cell lymphopenia in California: results of the first 2 years
Abstract
Background: Assay of T-cell receptor excision circles (TRECs) in dried blood spots obtained at birth permits population-based newborn screening (NBS) for severe combined immunodeficiency (SCID).
Objective: We sought to report the first 2 years of TREC NBS in California.
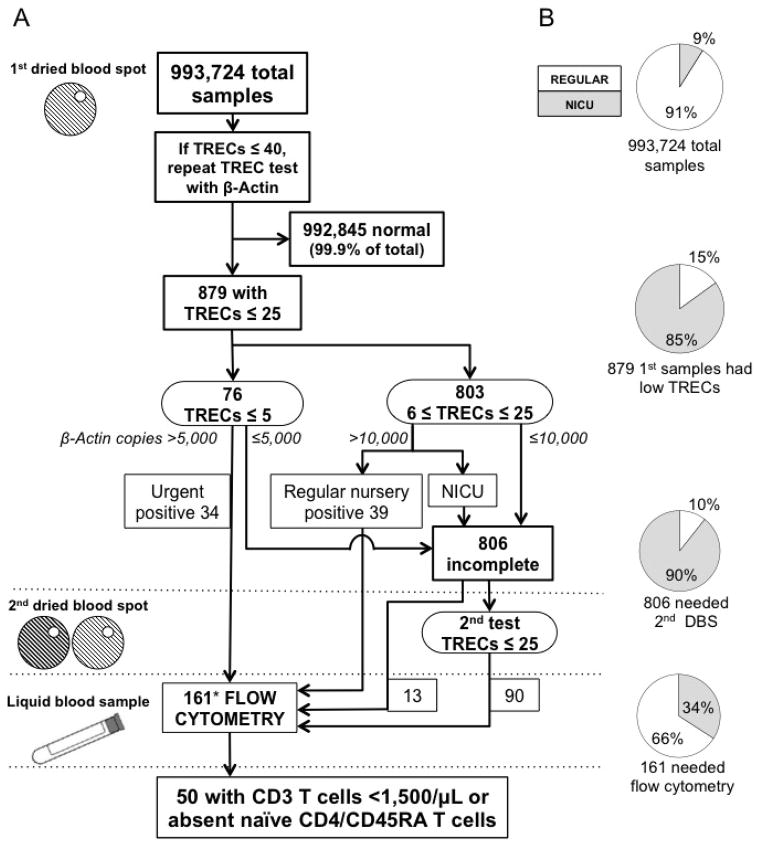
Methods: Since August 2010, California has conducted SCID NBS. A high-throughput TREC quantitative PCR assay with DNA isolated from routine dried blood spots was developed. Samples with initial low TREC numbers had repeat DNA isolation with quantitative PCR for TRECs and a genomic control, and immunophenotyping was performed within the screening program for infants with incomplete or abnormal results. Outcomes were tracked.
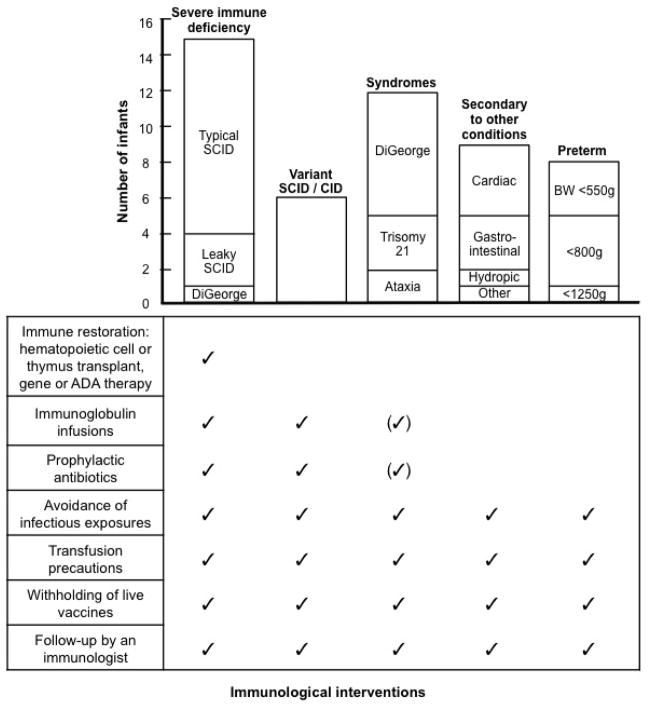
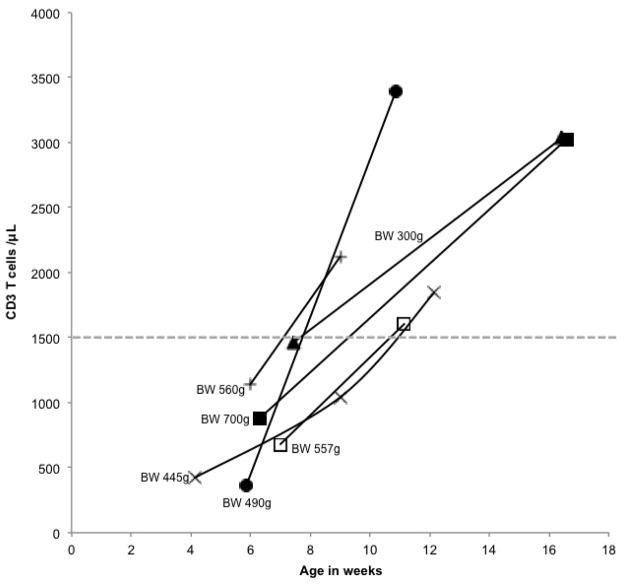
Results: Of 993,724 infants screened, 50 (1/19,900 [0.005%]) had significant T-cell lymphopenia. Fifteen (1/66,250) required hematopoietic cell or thymus transplantation or gene therapy; these infants had typical SCID (n = 11), leaky SCID or Omenn syndrome (n = 3), or complete DiGeorge syndrome (n = 1). Survival to date in this group is 93%. Other T-cell lymphopenic infants had variant SCID or combined immunodeficiency (n = 6), genetic syndromes associated with T-cell impairment (n = 12), secondary T-cell lymphopenia (n = 9), or preterm birth (n = 8). All T-cell lymphopenic infants avoided live vaccines and received appropriate interventions to prevent infections. TREC test specificity was excellent: only 0.08% of infants required a second test, and 0.016% required lymphocyte phenotyping by using flow cytometry.
Conclusions: TREC NBS in California has achieved early diagnosis of SCID and other conditions with T-cell lymphopenia, facilitating management and optimizing outcomes. Furthermore, NBS has revealed the incidence, causes, and follow-up of T-cell lymphopenia in a large diverse population.
Copyright © 2013 American Academy of Allergy, Asthma & Immunology. Published by Mosby, Inc. All rights reserved.
Figures
References
-
- Railey MD, Lokhnygina Y, Buckley RH. Long-term clinical outcome of patients with severe combined immunodeficiency who received related donor bone marrow transplants without pretransplant chemotherapy or post-transplant GVHD prophylaxis. The Journal of pediatrics. 2009;155(6):834–40. e1. - PMC - PubMed
-
- Adeli MM, Buckley RH. Why newborn screening for severe combined immunodeficiency is essential: a case report. Pediatrics. 2010;126(2):e465–9. - PubMed
-
- Brown L, Xu-Bayford J, Allwood Z, Slatter M, Cant A, Davies EG, et al. Neonatal diagnosis of severe combined immunodeficiency leads to significantly improved survival outcome: the case for newborn screening. Blood. 2011;117(11):3243–6. - PubMed
-
- Myers LA, Patel DD, Puck JM, Buckley RH. Hematopoietic stem cell transplantation for severe combined immunodeficiency in the neonatal period leads to superior thymic output and improved survival. Blood. 2002;99(3):872–8. - PubMed
Publication types
MeSH terms
Grants and funding
- AI U54 082973/AI/NIAID NIH HHS/United States
- R13 AI094943/AI/NIAID NIH HHS/United States
- R01 AI078248/AI/NIAID NIH HHS/United States
- U54 AI082973/AI/NIAID NIH HHS/United States
- UL1 RR024131/RR/NCRR NIH HHS/United States
- 1UL1 RR024131/RR/NCRR NIH HHS/United States
- R03 HD 060311/HD/NICHD NIH HHS/United States
- HHSN267200603430C/PHS HHS/United States
- N01 AI030070/AI/NIAID NIH HHS/United States
- R03 HD060311/HD/NICHD NIH HHS/United States
- R01 AI105776/AI/NIAID NIH HHS/United States
- R01 AI 078248/AI/NIAID NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
