

In vivo diagnosis of plaque erosion and calcified nodule in patients with acute coronary syndrome by intravascular optical coherence tomography
- PMID: 23810884
- PMCID: PMC3874870
- DOI: 10.1016/j.jacc.2013.05.071
In vivo diagnosis of plaque erosion and calcified nodule in patients with acute coronary syndrome by intravascular optical coherence tomography
Abstract
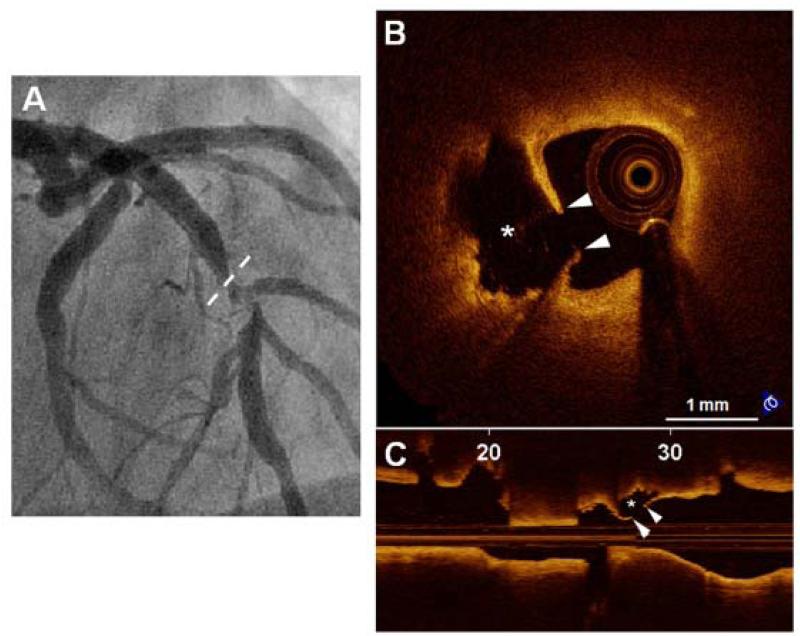
Objectives: The aim of this study was to characterize the morphological features of plaque erosion and calcified nodule in patients with acute coronary syndrome (ACS) by optical coherence tomography (OCT).
Background: Plaque erosion and calcified nodule have not been systematically investigated in vivo.
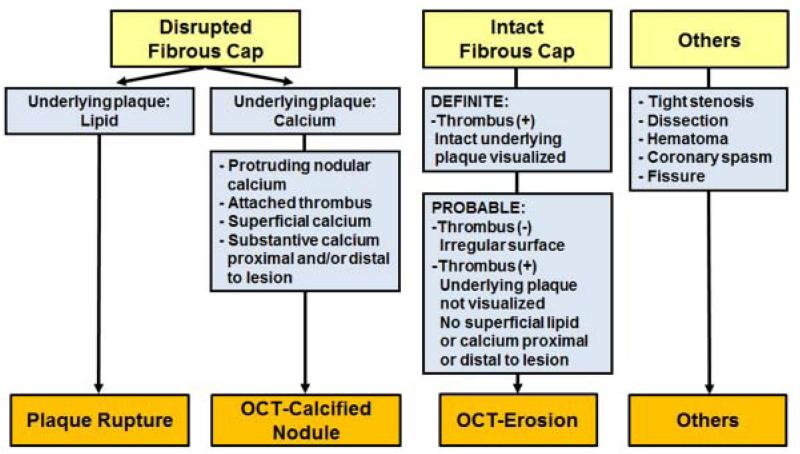
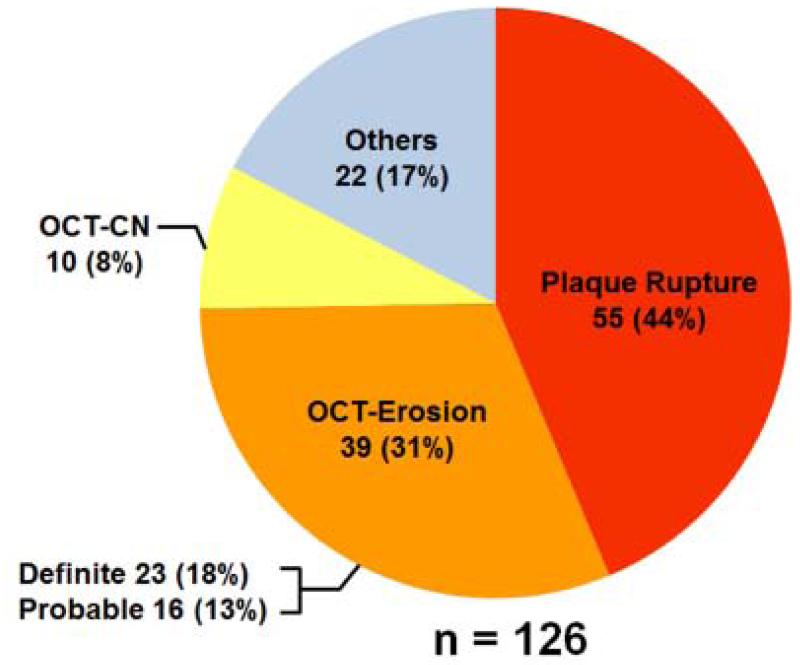
Methods: A total of 126 patients with ACS who had undergone pre-intervention OCT imaging were included. The culprit lesions were classified as plaque rupture (PR), erosion (OCT-erosion), calcified nodule (OCT-CN), or with a new set of diagnostic criteria for OCT.
Results: The incidences of PR, OCT-erosion, and OCT-CN were 43.7%, 31.0%, and 7.9%, respectively. Patients with OCT-erosion were the youngest, compared with those with PR and OCT-CN (53.8 ± 13.1 years vs. 60.6 ± 11.5 years, 65.1 ± 5.0 years, p = 0.005). Compared with patients with PR, presentation with non-ST-segment elevation ACS was more common in patients with OCT-erosion (61.5% vs. 29.1%, p = 0.008) and OCT-CN (100% vs. 29.1%, p < 0.001). The OCT-erosion had a lower frequency of lipid plaque (43.6% vs. 100%, p < 0.001), thicker fibrous cap (169.3 ± 99.1 μm vs. 60.4 ± 16.6 μm, p < 0.001), and smaller lipid arc (202.8 ± 73.6° vs. 275.8 ± 60.4°, p < 0.001) than PR. The diameter stenosis was least severe in OCT-erosion, followed by OCT-CN and PR (55.4 ± 14.7% vs. 66.1 ± 13.5% vs. 68.8 ± 12.9%, p < 0.001).
Conclusions: Optical coherence tomography is a promising modality for identifying OCT-erosion and OCT-CN in vivo. The OCT-erosion is a frequent finding in patients with ACS, especially in those with non-ST-segment elevation ACS and younger patients. The OCT-CN is the least common etiology for ACS and is more common in older patients. (The Massachusetts General Hospital Optical Coherence Tomography Registry; NCT01110538).
Keywords: ACS; ECG; MI; NSTE-ACS; NSTEMI; OCT; SCD; ST-segment elevation myocardial infarction; STEMI; acute coronary syndrome; acute coronary syndrome(s); calcified nodule; electrocardiogram; myocardial infarction; non–ST-segment elevation acute coronary syndrome; non–ST-segment elevation myocardial infarction; optical coherence tomography; plaque erosion; plaque rupture; sudden cardiac death.
Copyright © 2013 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Intracoronary optical coherence tomography: are we getting too close to the light?J Am Coll Cardiol. 2013 Nov 5;62(19):1759-60. doi: 10.1016/j.jacc.2013.06.011. Epub 2013 Jun 27. J Am Coll Cardiol. 2013. PMID: 23810868 No abstract available.
-
New insights on plaque erosion and calcified nodules: "seeing is believing".J Am Coll Cardiol. 2014 Apr 15;63(14):1458-9. doi: 10.1016/j.jacc.2013.08.1653. Epub 2013 Dec 4. J Am Coll Cardiol. 2014. PMID: 24315900 No abstract available.
-
We should use the OCT-based clinical term "acute coronary syndrome with intact fibrous cap (ACS-IFC)" rather than the pathology term "plaque erosion".J Am Coll Cardiol. 2014 Jun 24;63(24):2745. doi: 10.1016/j.jacc.2013.09.087. Epub 2014 Apr 23. J Am Coll Cardiol. 2014. PMID: 24768886 No abstract available.
References
-
- Virmani R, Kolodgie FD, Burke AP, Farb A, Schwartz SM. Lessons from sudden coronary death: a comprehensive morphological classification scheme for atherosclerotic lesions. Arterioscler Thromb Vasc Biol. 2000;20:1262–75. - PubMed
-
- Naghavi M, Libby P, Falk E, et al. From vulnerable plaque to vulnerable patient: a call for new definitions and risk assessment strategies: Part I. Circulation. 2003;108:1664–72. - PubMed
-
- Virmani R, Burke AP, Farb A, Kolodgie FD. Pathology of the vulnerable plaque. J Am Coll Cardiol. 2006;47:C13–8. - PubMed
-
- Davies MJ. Anatomic features in victims of sudden coronary death. Coronary artery pathology. Circulation. 1992;85:I19–24. - PubMed
-
- van der Wal AC, Becker AE, van der Loos CM, Das PK. Site of intimal rupture or erosion of thrombosed coronary atherosclerotic plaques is characterized by an inflammatory process irrespective of the dominant plaque morphology. Circulation. 1994;89:36–44. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
