

Clinical profile and underdiagnosis of pulmonary hypertension in US veteran patients
- PMID: 23811965
- PMCID: PMC3894604
- DOI: 10.1161/CIRCHEARTFAILURE.112.000091
Clinical profile and underdiagnosis of pulmonary hypertension in US veteran patients
Abstract
Background: Pulmonary hypertension (PH) is a key contributor to cardiovascular morbidity and early mortality; however, reports are lacking on the epidemiology of PH in at-risk patient populations.
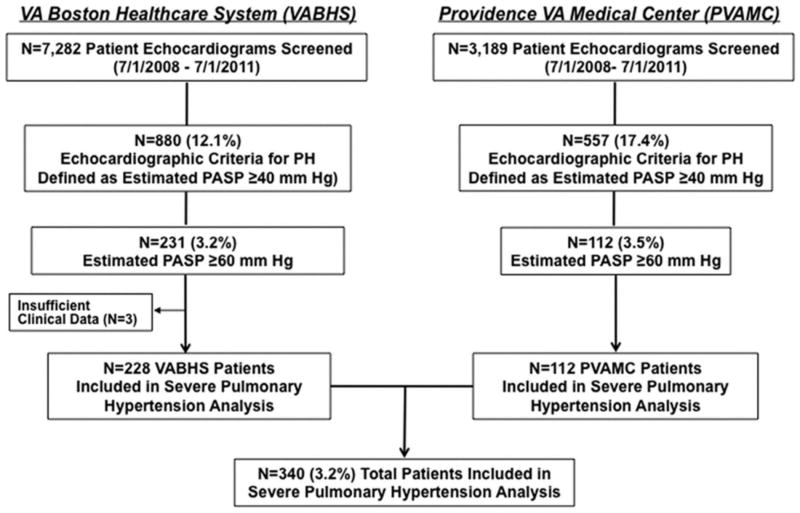
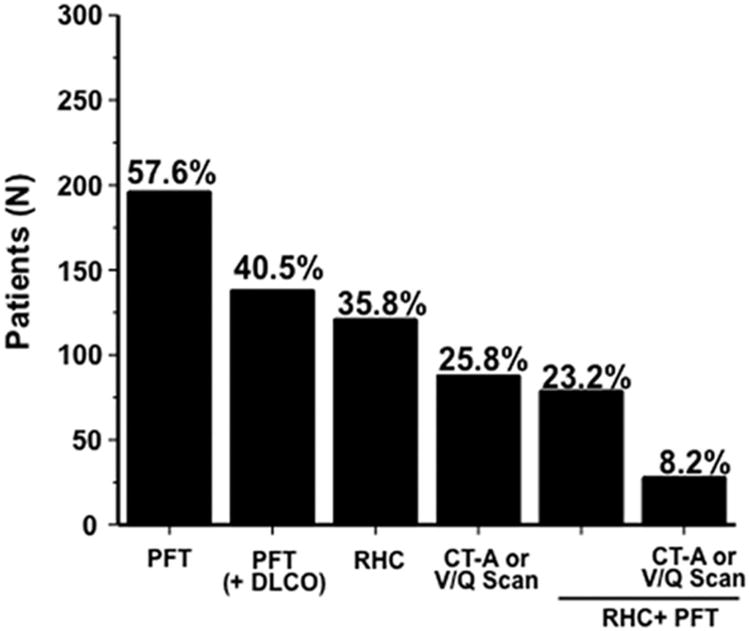
Methods and results: The echocardiography registries from 2 major Veterans Affairs hospitals were accessed to identify patients with at least moderate PH, defined here as a pulmonary artery systolic pressure ≥60 mm Hg detected echocardiographically. From a total of 10 471 individual patient transthoracic echocardiograms, we identified moderate or severe PH in 340 patients (332 men; mean, 77 years; mean pulmonary artery systolic pressure, 69.4±10.5 mm Hg), of which PH was listed as a diagnosis in the medical record for only 59 (17.3%). At a mean of 832 days (0-4817 days) following echocardiography diagnosing PH, 150 (44.1%) patients were deceased. PH was present without substantial left heart remodeling: the mean left ventricular ejection fraction was 0.50±0.16, left ventricular end-diastolic dimension was 5.0±0.9 cm, and left atrial dimension was 4.4±0.7 cm. Cardiac catheterization (n=122, 36%) demonstrated a mean pulmonary artery pressure of 40.5±11.4 mm Hg, pulmonary capillary wedge pressure of 22.6±8.9 mm Hg, and pulmonary vascular resistance of 4.6±2.9 Wood units. Diagnostic strategies for PH were variable and often incomplete; for example, only 16% of appropriate patients were assessed with a nuclear ventilation/perfusion scan for thromboembolic causes of PH.
Conclusions: in an at-risk patient population, PH is underdiagnosed and associated with substantial mortality. Enhanced awareness is necessary among practitioners regarding contemporary PH diagnostic strategies.
Keywords: diagnosis; epidemiology; pulmonary hypertension.
Conflict of interest statement
Figures
References
-
- Shah SJ. Pulmonary hypertension. JAMA. 2012;308:1366–1374. - PubMed
-
- Yu W, Ravelo A, Wagner TH, Phibbs CS, Bhandari A, Chen S, Barnett PG. Prevalence and costs of chronic conditions in the VA health care system. Med Care Res Rev. 2003;60:146S–167S. - PubMed
-
- Lanzarini L, Fontana A, Campana C, Klersy C. Two simple echo-Doppler measurements can accurately identify pulmonary hypertension in the large majority of patients with chronic heart failure. J Heart Lung Transplant. 2005;24:745–754. - PubMed
-
- Rudski LG, Lai WW, Afilalo J, Hua L, Handschumacher MD, Chandrasekaran K, Solomon SD, Louie EK, Schiller NB. Guidelines for the echocardiographic assessment of the right heart in adults: a report from the American Society of Echocardiography endorsed by the European Association of Echocardiography, a registered branch of the European Society of Cardiology, and the Canadian Society of Echocardiography. J Am Soc Echocardiogr. 2010;23:685–713. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
