

Phenotyping and outcome on contemporary management in a German cohort of patients with peripartum cardiomyopathy
- PMID: 23812247
- PMCID: PMC3709080
- DOI: 10.1007/s00395-013-0366-9
Phenotyping and outcome on contemporary management in a German cohort of patients with peripartum cardiomyopathy
Abstract
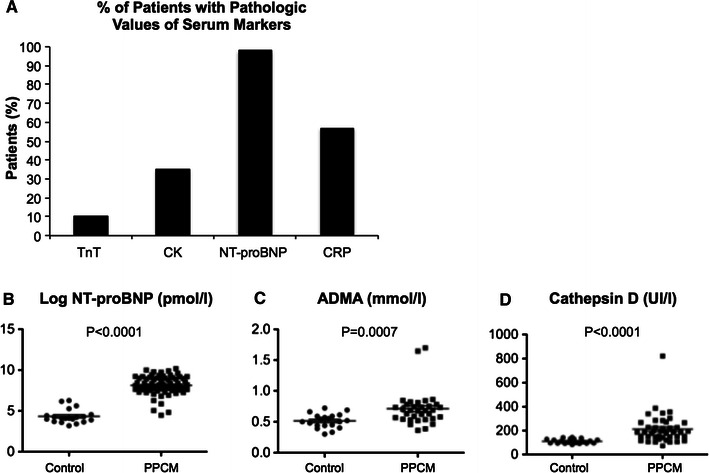
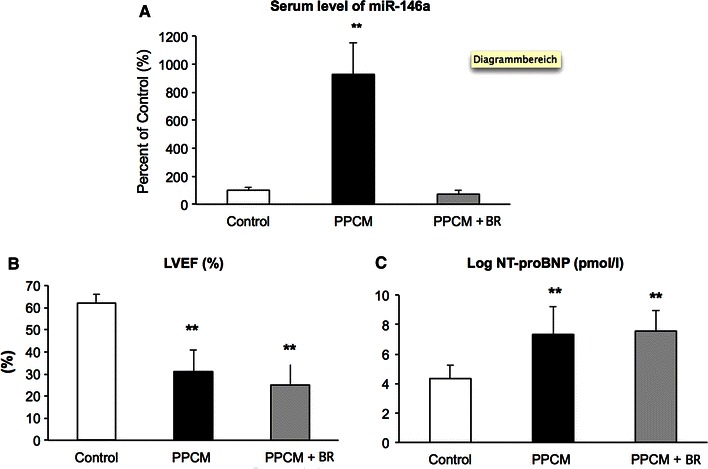
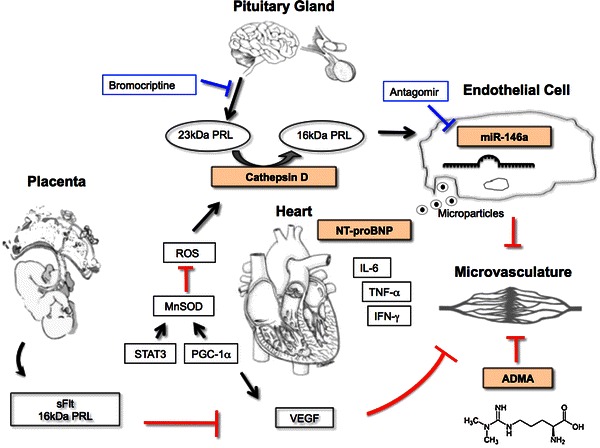
Peripartum cardiomyopathy (PPCM) is a life-threatening heart disease developing towards the end of pregnancy or in the months following delivery in previously healthy women in terms of cardiac disease. Enhanced oxidative stress and the subsequent cleavage of the nursing hormone Prolactin into an anti-angiogenic 16 kDa subfragment emerged as a potential causal factor of the disease. We established a prospective registry with confirmed PPCM present in 115 patients (mean baseline left ventricular ejection fraction, LVEF: 27 ± 9 %). Follow-up data (6 ± 3 months) showed LVEF improvement in 85 % and full recovery in 47 % while 15 % failed to recover with death in 2 % of patients. A positive family history of cardiomyopathy was present in 16.5 %. Pregnancy-associated hypertension was associated with a better outcome while a baseline LVEF ≤ 25 % was associated with a worse outcome. A high recovery rate (96 %) was observed in patients obtaining combination therapy with beta-blocker, angiotensin-converting enzyme (ACE) inhibitors/angiotensin-receptor-blockers (ARBs) and bromocriptine. Increased serum levels of Cathepsin D, the enzyme that generates 16 kDa Prolactin, miR-146a, a direct target of 16 kDa Prolactin, N-terminal-pro-brain-natriuretic peptide (NT-proBNP) and asymmetric dimethylarginine (ADMA) emerged as biomarkers for PPCM. In conclusion, low baseline LVEF is a predictor for poor outcome while pregnancy-induced hypertensive disorders are associated with a better outcome in this European PPCM cohort. The high recovery rate in this collective is associated with a treatment concept using beta-blockers, ACE inhibitors/ARBs and bromocriptine. Increased levels of Cathepsin D activity, miR-146a and ADMA in serum of PPCM patients support the pathophysiological role of 16 kDa Prolactin for PPCM and may be used as a specific diagnostic marker profile.
Figures
References
-
- Fett JD. Peripartum cardiomyopathy. Insights from Haiti regarding a disease of unknown etiology. Minn Med. 2002;85:46–48. - PubMed
-
- Forster O, Hilfiker-Kleiner D, Ansari AA, Sundstrom JB, Libhaber E, Tshani W, Becker A, Yip A, Klein G, Sliwa K. Reversal of IFN-gamma, oxLDL and prolactin serum levels correlate with clinical improvement in patients with peripartum cardiomyopathy. Eur J Heart Fail. 2008;10:861–868. doi: 10.1016/j.ejheart.2008.07.005. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
