

Paradoxical trends and racial differences in obstetric quality and neonatal and maternal mortality
- PMID: 23812453
- PMCID: PMC3701153
- DOI: 10.1097/AOG.0b013e3182932238
Paradoxical trends and racial differences in obstetric quality and neonatal and maternal mortality
Abstract
Objective: To evaluate trends by race in Agency for Healthcare Research and Quality obstetric-related quality and safety indicators and their relationships to trends in inpatient maternal and neonatal mortality.
Methods: We used the Nationwide Inpatient Sample from 2000 through 2009 and calculated obstetric hospital quality and patient safety indicators and inpatient maternal and neonatal mortality stratified by race. We examined differences in age and comorbidity-adjusted trends in black compared with white women over time in the United States and by geographic region. Proportions were analyzed by χ2 and trends by regression analysis.
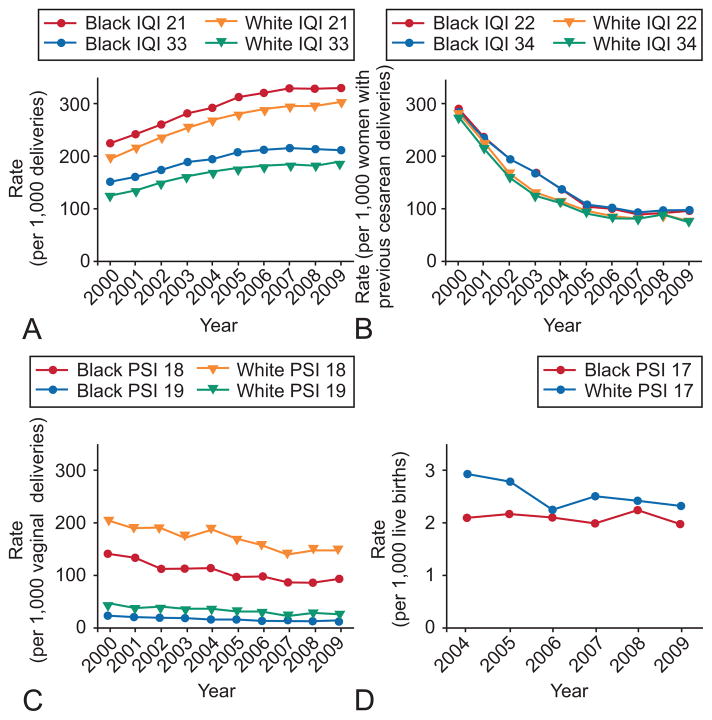
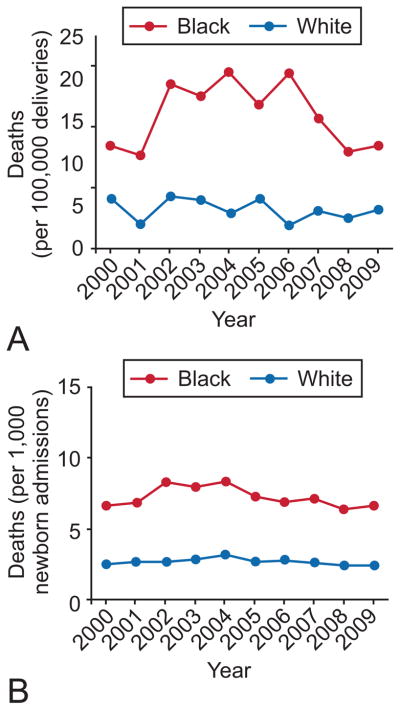
Results: Obstetric quality indicators varied by geographic region, but changes over time were consistent for both races. Cesarean deliveries increased similarly for black and white women, and vaginal births after cesarean delivery declined for both races but more rapidly for white women than for black women. Obstetric safety indicators improved over the study period for black and white women, with obstetric trauma decreasing significantly for both groups (28% compared with 35%, respectively) and birth trauma-injury to neonates declining for both, but changes were not significant. In striking contrast, inpatient maternal and neonatal mortality remained relatively constant during the study period, with persistently higher rates of both seen among black compared with white women (12.0 compared with 4.6 per 100,000 deliveries, P<.001 and 6.6 compared with 2.5 per 1,000 births, P<.001, respectively, in 2009).
Conclusion: Improvements in Agency for Healthcare Research and Quality quality indicators for obstetrics are not reflected in improvements in maternal and neonatal morbidity and mortality and do not explain continued racial disparities for outcomes in pregnancies in black and white women. Quality measures that are related to pregnancy outcomes are needed and these should elucidate obstetric health disparities.
Figures
References
-
- Martin JA, Hamilton BE, Sutton PD, Ventura SJ, Menacker F, Kirmeyer S. Births: final data for 2004. Natl Vital Stat Rep. 2006;55:1–101. - PubMed
-
- Andrews RM. HCUP Statistical Brief 59. Rockville, MD: Agency for Healthcare, Research, and Quality; 2008. The national hospital bill: the most expensive conditions by payer, 2008. - PubMed
-
- Asch DA, Nicholson S, Srinivas S, Herrin J, Epstein AJ. Evaluating obstetrical residency programs using patient outcomes. JAMA. 2009;302:1277–83. - PubMed
-
- Gregory KD, Fridman M, Shah S, Korst LM. Global measures of quality- and patient safety-related childbirth outcomes: should we monitor adverse or ideal rates? Am J Obstet Gynecol. 2009;200:681 e1–7. - PubMed
-
- Srinivas SK, Epstein AJ, Nicholson S, Herrin J, Asch DA. Improvements in US maternal obstetrical outcomes from 1992 to 2006. Med Care. 2010;48:487–93. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
